2022.07.02.31
Files > Volume 7 > Vol 7 No 2 2022

Eman Wahab Kadhum1,*  , Basim Mohammed Hanon2*
, Basim Mohammed Hanon2*
1* Department of Dentistry, Al-Mustaqbal University College, Hilla, Babil, Iraq.
2* Department of Microbiology, College of Veterinary Medicine, University of Wasit.
Corresponding author: Basim Mohammed Hanon
Available from: http://dx.doi.org/10.21931/RB/2022.07.02.31
ABSTRACT
Background: psoriasis is a prevalent, persistent, non - contagious skin disorder of unknown origin or cure. It has a significant detrimental influence on people’s life. It was hypothesized that there is a relation between reducing vitamin D levels and psoriasis. Psoriasis is a severe global condition that affects at least 100 million people; the incidence of psoriasis ranges from 0.09 to 11.43 %. The incidence of psoriasis is 0.09 % to 11.43 %. Objectives & Methodology: Study the frequency of and incidence of psoriasis and its correlation with serum vitamin D3 level; 150 people aged between 1-45 years old and from both sexes were selected for the current study. All of them were recruited from Hilla Teaching Hospital and TelAfer from November 2018 to February 2019 in Babylon Governorate. Of them, 50 were suffering from Psoriasis symptoms, 50 were presented with a positive family history of psoriasis, and the last 50 people were healthy and considered a control group. They were all subjected to estimating the serum level of vitamin D3 by using the ELISA technique. Results: a significant decrease in the serum level of vitamin D3 was found among patients with psoriasis compared to the control and family history groups. The study also indicates that the onset frequency of psoriasis has a hereditary component.
In comparison to the age groups (1-15) and (16-30), the results showed a considerable increase in the age groups (31-45). The incidence was more in males than in females. Conclusions: A significant decrease in vitamin D3 in patients with psoriasis.
Keywords. family history, gender types, Vitamin D3, psoriasis
INTRODUCTION
Psoriasis is a common, persistent, non - contagious skin disease with an unknown cause or cure. It has a significant detrimental influence on people’s life. Psoriasis influences people of different ages in every country. Psoriasis is a severe global condition that affects about 100 million persons. The estimated incidence of psoriasis is from 0.09 % to 11.43 %.1
Psoriasis symptoms are unexpected, and there are a lot of extrinsic triggers and significant comorbidities, like arthritis, heart disease, metabolic syndrome, depression, and inflammatory bowel disease.2
The etiology of this illness is undefined, with emerging evidence of a genetic predisposition.3 The role of immunity in the development of psoriasis is also a hot topic in research. Although it has been suggested that psoriasis is an autoimmune illness, no autoantigen has yet been identified as the cause. Extrinsic and intrinsic factors involving moderate trauma, sunlight, infections, systemic medicines, and stress can cause psoriasis.4
Psoriasis affects the nails and skin, and it’s linked to a slew of other conditions. Localized or widespread skin lesions are usually symmetrical, with crimson papules and plaques with highly defined borders that are typically covered in white or silver scales. Itching, stinging, and pain are all symptoms of lesions.5 Psoriasis was reported to have increased from 4.8 percent in 1979-1980 to 11.4 percent in 2007-2008. Recent research has revealed a rise in the prevalence of psoriasis; between the 1970s and 2000, the number of instances roughly doubled, with the cause still unknown.2 the study aims to explain the correlation between vitamin D3 levels.
MATERIALS AND METHODS
Study population
The study included three groups of people (50 persons in each group) who attended Hilla Teaching Hospital in Babil Governorate and TelAfer during the period (Nov. 2018 – Feb. 2019), their ages were between (1-45) years old and both genders. Of the fifteen patients suffering from a skin lesion and dermatitis, fifteen persons have a positive family history of psoriasis. The last fifteen were healthy as a control group. They were divided into three age groups (1-15, 16-30, and 31-45). By excluding any healthy control with the abnormal value of vitamin D.
Study samples
Three ml of venous blood samples were collected from the study participants in sterile coagulation tubes and then left for (60 min) at room temperature (25C˚). Blood samples were centrifuged at 3000 rpm for 15 minutes to obtain serum. The serum samples were used for the estimation of vitamin D3 levels.
Estimation of serum vitamin D3 level
Serum samples obtained from the study populations were subjected to determining vitamin D3 levels. Enzyme-Linked Immune Fluorescent Assay technique was depended for this purpose by using VIDAS 25 OH Vitamin D total kit performed by (bioMérieux SA, 376 Chemin de l’Orme,
69280 Marcy-l'Etoile – France).
Statistical Analysis
Study results were analyzed by using SPSS software package version 23 (performed by IBM Com. the USA). Chi-square and t-test were used in the analysis considering a P-value of ≤ 0.05 as a significance level.
RESULTS
Serum vitamin D3 Level
The results of the current study found a significant decrease (P-value < 0.01) in the level of serum vitamin D3 in psoriasis patients and family history groups compared to the healthy persons (control group) as presented in figure (1). According to the age group, figure (2) shows that serum vitamin D3 levels also decreased significantly in all age groups of psoriasis patients and family history groups compared to the control group.
.
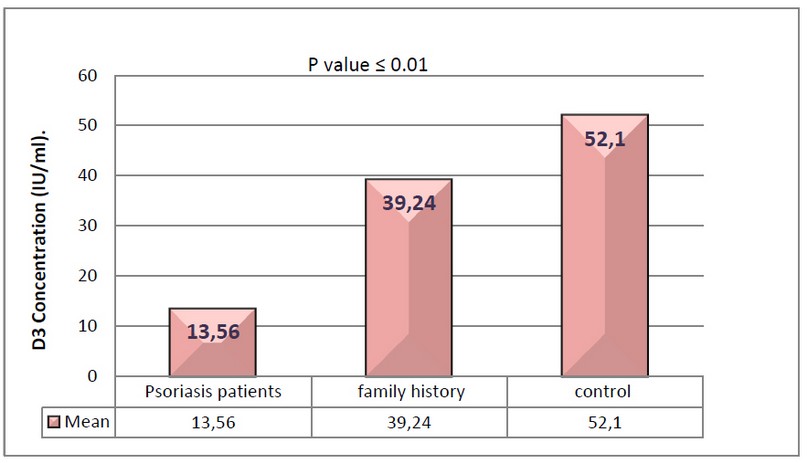
Figure 1. Mean vitamin D3 concentration in psoriasis patients, family history groups and control group
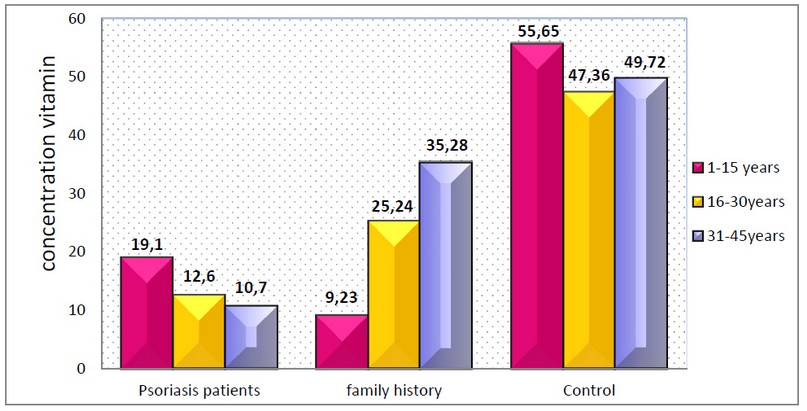
Figure 2: Mean vitamin D3 concentration concerning age among the study groups
The Relationship between vitamin D3 and the gender
A considerable drop in vitamin D3 was found in this study among psoriasis patients and family history groups compared to the control group and for all age groups and both genders.
Both genders presented a statistically considerable decrease in the level of vitamin D3 among psoriasis patients (16.15±13.9 IU/ml for males and 9.07±1.50 IU/ml for females) in the first age group 1-15years old (p<0.01) compared to the control group as presented in table (1). Similar decreasing the level of serum vitamin D3 levels were also found in the age groups (16-30 and 31-45 years old). These results were also statistically significant (p<0.01and p<0.05). However, we noticed that the serum vitamin D3 level was higher in psoriasis males from the age group (1-15years old), which was the opposite of the vitamin level of healthy people belonging to the same age group. For the other age groups, psoriasis females had higher levels of vitamin D3 level compared to psoriasis males; these results were utterly inverted in the healthy subjects from the same age groups, table (1).
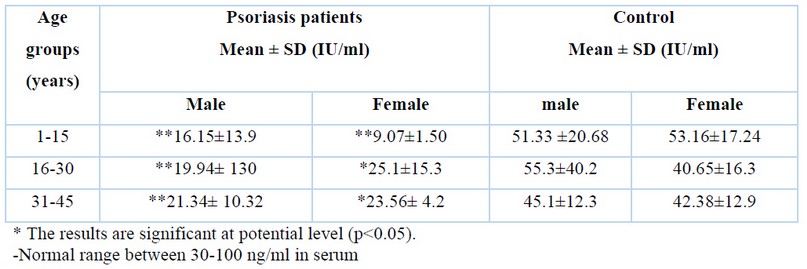
Table 1. The relationship between gender and age with vitamin D3 concentration in psoriasis patients and control group
Similarly, table (2) showed that the family history group also had lower serum vitamin D3 levels compared to healthy groups for both genders and all age groups involved in the present study. Differences exist between the vitamin D3 levels according to the age and sexes among family history persons and a control group.
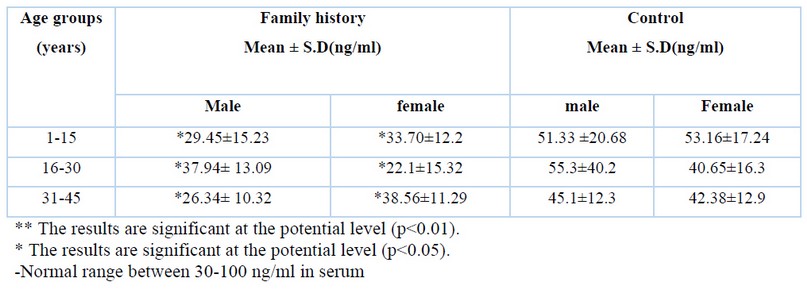
Table 2. The relationship between gender and age with vitamin D3 concentration in family history groups and control group
Types of psoriasis
Out of (50) psoriasis patients that were included in this study, it was found (73.3%) of the cases were positive for plaque psoriasis type, followed by (20%) with inverse psoriasis and (6.7%) nail psoriasis.
There was a highly significant association between plaque psoriasis type compared to other types of psoriasis among psoriasis patients (P < 0.01), as seen in the table (3).
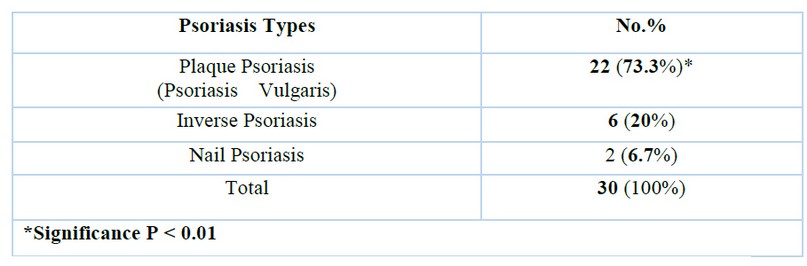
Table 3. Frequencies of psoriasis types in studied patients.
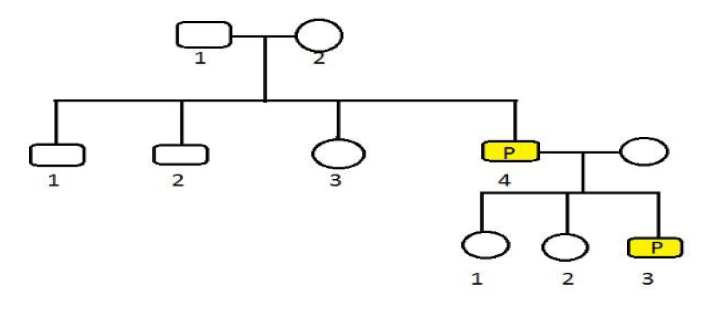
Figure 3. Pedigree Analysis for family
DISCUSSION
Vitamin D3
Our study proved that vitamin D3 is low when psoriasis patients are severely reduced; this proves that psoriasis associated with vitamin D3 compared with control suggests that the control result was expected. The usual range of vitamin D3 in the human body, since possessing a level of less than 10 ng/ml, indicates a severe deficiency, while reading ranging from 10 - 25 ng/ml suggests an average lack. If reading between 25 - 85 ng/ml is considered adequate and normal for healthy people.6 In both groups (controls and patients), blood 25-hydroxycholecalciferol levels remained below the standard limit suggested by the American Society for Bone and Mineral Research. Patients with psoriasis had significantly lower levels of 25-hydroxycholecalciferol than healthy people, with the lowest level coming from patients with severe psoriasis.7 The blood levels of 25 (OH) D in psoriatic patients were substantially lower (21.8ng/mL) than in healthy controls (34.3ng/mL). 8
Frequency of psoriasis in different sexes and age groups
Psoriasis and its relationship with sex did not notice a significant variation in the incidence of psoriasis in both sexes. Psoriasis does not affect the specific sex; both sexes are vulnerable to psoriasis. The males who enrolled in the present study were 19, while the female was 11; the severity of psoriasis was similar according to age and gender. Compared to patients aged between 46 to over -65 years old, patients aged 18 to 29 and 30-to-45 showed higher frequently (P-value more than 0.05) concerns with appearance/socialization and occupation/finances. Men reported more work-related stress than women did, although there were no gender differences in the frequency of items related to appearances and socialization (P-value more than 0.05). 9 This disease is common among Caucasians, affecting an estimated 125 million people worldwide. 10 Psoriasis influences about 3% of the population and affects men and women equally, with a 1:1 female to male ratio of 11,12 . Psoriasis Vulgaris, which accounts for about 90% of all cases, is distinguished by well-defined, dark red, scaly lesions and plaques, usually appearing on the elbows, knees, scalp and other skin areas. 13 Chronic plaque is the most common type of psoriasis, accounting for approximately 70% to 80% of all patients. 14 Griffiths et al.15 also stated that persistent plaque psoriasis was the most common type of psoriasis. The most prevalent clinical phenotype was chronic plaque-type psoriasis, with guttate and erythrodermic variations accounting for fewer than 2% of all cases.16
According to Kumar et al.17, the most common pattern of involvement was plaque psoriasis type lesions located over pressure bearing areas on the palms, and isolated plaques present randomly over the soles. Over five years, Kaur et al. 18 investigated nail alterations in 167 psoriasis patients. Of the overall cases, 3% showed isolated nail involvement. Inverse psoriasis is an uncommon type that affects about 3% to 7% of people living with psoriasis.19 Psoriasis Vulgaris was shown to be more common on the Iberian Peninsula, according to a study (79.8 %).20 Another Japanese study of nearly 28000 psoriasis patients found that 86.0 % had plaque psoriasis, and 2.8 percent had guttate psoriasis.21 Psoriasis affects more than 2% worldwide, with guttate psoriasis accounting for 2% of these instances.22
Frequency psoriasis in families of patients and analysis of the genealogy
Family history and effect on psoriasis of family history has an apparent impact on psoriasis, which is also a genetic disease. We have noticed this through the collected samples, and they were infected with psoriasis, of which about 70% have a family history. This result indicates that psoriasis has a strong relationship with inheritance. We have demonstrated this relationship through the work of the family tree of the disease. For a long time, psoriasis has been known to run in families. In his famous epidemiological research of psoriasis among 10,000 residents of the Faroe Islands, Lomholt discovered that the prevalence of psoriasis was much greater among first- and second-degree relatives of sufferers than among unaffected control persons.23 Another way to look into the heredity and penetrance of a disease is to compare illness concordance in monozygotic (MZ) twins (who have identical genomes) and dizygotic (DZ) twins (who only share half of their genomes). The heritability of psoriasis, h2 (the amount of phenotypic variation of a variable attributed to genetic differences), ranges from 60% to 90% based on twin and family studies, making it one of the highest for all multifactorial genetic illnesses. Psoriasis concordance in MZ twins is increased substantially compared with DZ twins, suggesting a genetic predisposition to the disease.24,25
CONCLUSIONS
Many theories have been proposed to explain the inheritance of psoriasis. Earlier, It hypothesized a dominant inheritance model with imperfect penetration. Psoriasis is thought to be inherited in a complex manner nowadays. Psoriasis’ genetic contribution has been widely characterized, with at least 20 distinct psoriasis susceptibility loci identified.26
Author contribution and funding
AM designed the tables and supervised and reviewed the manuscript, RM drafted the manuscript and compiled information from the literature. There is no source of funding, and the authors bear the expenses.
Ethics statement
This study was done in conformity with the testament of the committee of ethical standards in the College of Science, University of Al-Mustaqbal University College. Babylon Governorate.
REFERENCES
1. Danielsen, K., Olsen, A. O., Wilsgaard, T., & Furberg, A. S. Is the prevalence of psoriasis increasing? A 30‐year follow‐up of a population‐based cohort. British Journal of Dermatology. 2013. 168(6), 1303-1310.
2. Stănescu, A. M. A., Matei, A., Grăjdeanu, I. V., Appiah, E. A., Paparău, C., & Giurcăneanu, C. Asocierea între psoriazis şi sindromul metabolic, corelată cu deficitul vitaminei D în ambele afecţiuni. Revista Medicală Română. 2016. 1, 81-85.
3. Harden, J. L., Krueger, J. G., & Bowcock, A. M. The immunogenetics of psoriasis: a comprehensive review. Journal of autoimmunity. 2015. 64, 66-73.
4. Boehncke, W. H. Systemic inflammation and cardiovascular comorbidity in psoriasis patients: causes and consequences. Frontiers in immunology. 2018. 9, 579.
5. Parisi, R., Symmons, D. P., Griffiths, C. E., & Ashcroft, D. M. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. Journal of Investigative Dermatology. 2013. 133(2), 377-385.
6. Kovács, S., Wilkens, M. R., & Liesegang, A. Influence of UVB exposure on the vitamin D status and calcium homoeostasis of growing sheep and goats. Journal of animal physiology and animal nutrition. 2015. 99, 1-12.
7. Barrea, L., Nappi, F., Di Somma, C., Savanelli, M., Falco, A., Balato, A., ... & Savastano, S. Environmental risk factors in psoriasis: the point of view of the nutritionist. International journal of environmental research and public health. 2016. 13(7), 743.
8. Suskind, D. L., Cohen, S. A., Brittnacher, M. J., Wahbeh, G., Lee, D., Shaffer, M. L., ... & Giefer, M. Clinical and fecal microbial changes with diet therapy in active inflammatory bowel disease. Journal of clinical gastroenterology. 2018. 52(2), 155.
9. Gupta, M. A., & Gupta, A. K. Psoriasis and sex: a study of moderately to severely affected patients. International Journal of Dermatology. 1997. 36(4), 259-262
10. Langley, R. G. B., Krueger, G. G., & Griffiths, C. E. M. Psoriasis: epidemiology, clinical features, and quality of life. Annals of the rheumatic diseases. 2005. 64(suppl 2), ii18-ii23.
11. Duarte, G. V.; Follador, I.; Cavalheiro, C. M. A.; Silva, T. S. and De Oliveira, M. D. S. P. Psoriasis and obesity: literature review and recommendations for management. An. Bras. Dermatol. 2010. 85(3): 355-360.
12. Abbas, A. K., Lichtman, A. H., & Pillai, S. Cellular and molecular immunology E-book. Elsevier Health Sciences. 2013.
13. Coimbra, S.; Oliveira, H.; Figueiredo, A.; Rocha-Pereira, P. and Santos-Silva, A. Psoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial Aspects. 2012. Psor. Syste. Dise.: 71.
14. Naldi, L., Chatenoud, L., Piccitto, R., Colombo, P., Placchesi, E. B., & La Vecchia, C. Prevalence of actinic keratoses and associated factors in a representative sample of the Italian adult population: Results from the Prevalence of Actinic Keratoses Italian Study, 2003-2004. Archives of dermatology. 2004. 142(6), 722-726.
15. Griffiths, C.E.M.; Camp, RDR and Barker JNWN Psoriasis. In: Rook’s Textbook of Dermatology (Burns DA, Breathnach SM, Cox NH, Griffiths CEM, eds), 7th edn. 2004. Oxford: Blackwell Science.
16. Kaur, I.; Handa, S. and Kumar, B. Natural history of psoriasis: a study from the Indian subcontinent. J. Dermatol. 1997. 24 (4): 230-234.
17. Kumar, B.; Saraswat, A. and Kaur, I. Palmoplantar lesions in psoriasis: A study of 3065 patients. Acta. Derm. Venereol. 2002. 82(3):192-195.
18. Kaur, I.; Saraswat, A. and Kumar, B. Nail changes in psoriasis: a study of 167 patients. Int. J. Dermatol. 2001. 40 (9): 601-603.
19. Syed, Z. U., & Khachemoune, A. Inverse psoriasis. American journal of clinical dermatology. 2011. 12(2), 143-146.
20. Garcia-Diez, A.; Foraster, C.F.; Sebastian, F.V.; Tudela, LL; Llach, X.B. and Fernandez, G.S. What characterizes the severity of psoriasis? Results from an epidemiological study of over 3,300 patients in the Iberian region. Dermatol. 2008.. 216 (2): 137-151.
21. Kawada, A.; Tezuka, T.; Nakamizo, Y.; Kimura, H.; Nakagawa, H. and Igarashi, A. Japanese Society for Psoriasis Research. A survey of psoriasis patients in Japan from 1982 to 2001. J. Dermatol. Sci. 2003. 31 (1): 59-64.
22. Telfer, N. R., Chalmers, R. J., Whale, K., & Colman, G. The role of streptococcal infection in the initiation of guttate psoriasis. Archives of dermatology. 1992. 128(1), 39-42.
23. Lønnberg, A. S., Skov, L., Skytthe, A., Kyvik, K. O., Pedersen, O. B., & Thomsen, S. F. Heritability of psoriasis in a large twin sample. British Journal of Dermatology. 2013. 169(2), 412-416.
24. Lønnberg, A. S., Skov, L., Duffy, D. L., Skytthe, A., Kyvik, K. O., Pedersen, O. B., & Thomsen, S. F. Genetic factors explain variation in the age at onset of psoriasis: a population-based twin study. Acta dermato-venereologica. 2016. 96(1), 35-38.
25. Solmaz, D., Ureyen, S. B., Kimyon, G., et al. THU0285 The effect of family history on disease phenotypes in 1393 psoriatic arthritis patients. Ann Rheum Dis. 2018. 77(2):361.1-361
26. Friberg, C. Genetic studies of psoriasis and psoriatic arthritis. Inst of Biomedicine.. Dept of Medical Genetics. 2007 Camilla Friberg. ISBN: 978-91-628-7286-1.
Received: 30 December 2021 / Accepted: 23 February 2022 / Published:15 May 2022
Citation: Eman Wahab Kadhum E, Mohammed Hanon B. Serological estimation of serum level of Vitamin D3 among Psoriasis patients. Revis Bionatura 2022;7(2) 31. http://dx.doi.org/10.21931/RB/2022.07.02.31