2019.04.03.12
Files > Volume 4 > Vol 4 No 3 2019
REVISION/REVIEW
Pembrolizumab and Nivolumab in the treatment of Non-small cell lung cancer (NSCLC).

Camila Lissett Velastegui Gamboa and Dayanara Lissette Yánez Arcos
Available from: http://dx.doi.org/10.21931/RB/2019.04.03.12
ABSTRACT
Lung cancer is a disease difficult to treat and with low survival rates, especially non-smaller cell lung cancer (NSCLC). To treat cancer in advanced stages, new methods had arisen like immunotherapy. Pembrolizumab and nivolumab are IgG4 antibodies targeting programmed death cell receptor (PD-1) used for cancer immunotherapy, that blocks the protection that has cancer cells against the immune system. This antibody works binding and blocking the PD-1 membrane protein of T cells, which is responsible for cell recognition. If T cells cannot recognize the cells, then it would attack, so in this way, the immune system can be enhanced. Pembrolizumab and nivolumab have a variable region that is capable of recognizing the PD-1 receptor, and this plays an important role to kill cancer cells. The structure of the complex PD -1 and its ligand PD-L1 or PD-L2 reveals the structural basis of the PD-1. The interaction with a human antibody has been studied with antibody fragments revealing the molecular basis for the blockade of PD1 / PDL1-PDL2 interaction by pembrolizumab and nivolumab. Different studies involving immunotherapy have shown the remarkable results of pembrolizumab and nivolumab over current chemotherapy for cancer treatment making available a possible way for a new treatment for lung cancer. In a comparative analysis made between those immune checkpoint inhibitors had found the efficacy of pembrolizumab for treatment of NSCLC.
Keywords: Pembrolizumab, nivolumab, lung cancer, immunotherapy
INTRODUCTION
Around the world, there is an increase of 18.1 million new cases of cancer and 9.6 million die from this disease in 2018. Of which, the cancers with the highest incidence are lung, breast, and colorectal cancer, in turn, are found among the top five with the highest mortality. Of these, lung cancer is found to have the highest mortality, with 1.8 million deaths. 1 In the United States, 1 735 350 new cases have been reported during 2018, of which 606640 will die from this disease 2. Currently, in the world, more than 32 million people suffer from this disease and will increase by 70% in the next 20 years 3. The World Health `Organization has defined cancer as one of the leading causes of deaths in the world, with lung cancer having the highest number of deaths with 1.69 million in 2015 4.
In Ecuador, it constitutes a serious public health problem, with a 20% chance of acquiring cancer before 75 years of age 5. Lung cancer is one of the most aggressive, being the one that produces the highest number of deaths per year, according to data from the National Registry of Tumors of the Fight Against Cancer Society in Ecuador (Solca), registering 384 deaths during 2014 and 753 deaths in 2012 6. The cancer mortality rate during 2009 and 2013 for bronchial lung cancer was 11.1% and an incidence rate of 14.4% 7.
To give a solution to the problem, new and more effective treatments have been developed. One of these treatments is immunotherapy. The food and drug administration (FAO) has approved several treatments for the treatment of cancer, like Nivolumab and Pembrolizumab for untreated metastatic non-squamous non-small lung cancer 8. The clinical trials of both had demonstrated an improvement in the overall response rate and progression-free survival 9,10. Nivolumab was the first PD-1 inhibitor to gain regulatory approval 9. By the other side, Pembrolizumab was nominated for the molecule of the year in 2017 for its promising results in the treatment of cancer, as well as its versatility in the treatment of several types of cancer, such as lung cancer 11. This review presents the data of Nivolumab and Pembrolizumab in the treatment of non-small cell lung cancer.
Types of small cell cancer
Lung cancer is one of the most common cancers and has the highest mortality rate of 12. At diagnosis, half of the patients die within one year, and the overall surviving rate in 5 years is approximately 17.8% 13. There are two main types of lung cancer: small cell lung cancer (SCLC) and non-small-cell lung cancer (NSCLC). The first account for 15% of lung cancer and 25% of deaths. This type of cancer tends to metastasize early, so operation is not useful and rarely used as treatment. Chemotherapy and radiotherapy are usually used for cancer treatment in SCLC, although the cure is not easy to achieve 14.
Non-small cell cancer is the most common type of cancer, accounting approximately 85 % of cancer diagnoses. This type of cancer is characterized by a different class of tumors 15 and can be subdivided into three main categories squamous-cell carcinoma, adenocarcinoma, and large-cell carcinoma.
Squamous-cell carcinoma accounts for 25%-30% of lung cancer and is characterized because it arrays in the epithelial cell of the bronchi. Adenocarcinoma account by 40% of all lung cancer, being the most common. This type tends to grow in peripheral of the lungs and grows slowly. Large-cell carcinoma is detected by the default of the two other possibilities because it did not show clear symptoms 13.
Types of treatment current used
The detection of stage cancer and the type of tumor are key steps at the moment to choose the treatment. Different treatment includes surgery, chemotherapy, radiotherapy, molecular targeting, and immunotherapy (15). Patients with NSCLC in stage I, II, and III commonly have surgery to remove the tumor, although to avoid the relapse, they also have chemotherapy and radiotherapy 16.
Approximately 40% of patients have stage IV, and there is not a cure for them due to in this stage, cancer had spread long distances. Their first line of treatment is the combination of chemotherapy based with both platinum and non-platinum compounds 17. The treatment will depend on the performance status (PS) that is a score that estimates the ability of the patient to do some activities 18. PS around 0 to 1 recommend platinum- doublet therapy. Patients with PS 2, recommend only one drug which is typically not platinum 19.
Radiotherapy also constitutes a type of treatment of patients with lung cancer. This treatment is important to avoid the locoregional recurrence. Because radiotherapy uses high energy to damage DNA in the cancer cell, it is used at specific sites of the body 20. Addition of radiotherapy to chemotherapy increases the survival in 3 years approximately 5% 14.
Another therapy that is improving the survival rate is the molecular targeting of cells, in which the target against some factor that helps tumors growth is avoided. The targets are for: epidermal growth factor receptor (EGFR) which is involved in cell growth and proliferation; KRAS a mutated gene present in NSCLC; anaplastic lymphoma kinase ALK which commonly is mutated in tumors; BRAF a proto-oncogene that regulates survival and cell proliferation 13.
Finally, one of the recent therapies that are applying is immunotherapy in which the own immune system can kill tumor cells. These cells present common characteristics that made them be recognized by the immune system and can avoid being destroyed 21. The edition of this mechanism made the cytotoxic cells able to destroy tumor cells. The problem with this therapy is that the immune system cannot identify the normal cells either, so it can also develop an autoimmune disease. In patients with advanced lung cancer is a matter of extent, their lifetime, because non-small cell lung cancer stage IV has no cure. This principle is the principle of work for pembrolizumab and nivolumab.
Immunotherapy treatment for lung cancer
Cancer cells have mutations that provide characteristic for being recognized like antigens, although, like cancer cells are cells of the body, it can also present characteristic that enables the immune system to attack. In the case of T cells, the amplitude of the response is mediated by the recognition of the T cell receptor (TCR). This recognition can be regulated by stimulatory and inhibitory signals knowing as immune checkpoints 22.
The inhibitory immune checkpoints control the function of T lymphocytes avoiding the excessive immune activation, and they are key factors in how cancer cells evade the immune system. Blockage of these immune checkpoints can enhance the activity of the T cell against cancer cells 23.
One of these immune checkpoints is the protein PD-1, that is like a gene encoding for a protein of the immunoglobulin superfamily. The expression of this gene was associated with dying thymocytes, so this protein was called programmed death receptor PD-1. After was shown that this protein is not involved in apoptosis and have an important role in immune cell tolerance; as a result, it prevents immune disease 24.
Mechanism of action
The immune system evasion is the headline procedure of cancer cell to reduce or limit the effectiveness of antitumor response of the immune system by 25 causing a localized immune suppression through activating of a key immune checkpoint 26. The structural information of this immune checkpoint protein and its complex with ligands, antibodies, has a potentiality ability for therapeutic designing agents in the immune checkpoint targeting of cancer 27. Effective therapies given by an adequate molecular recognition of cancer antigens benefit the rise of the new era of treatment, where the individual immune system evade the suppression and combat against them 28. For that, this next step is crucial in advance of bettering clinical responses in a combination of immunotarget therapy, and it is the focus in researches, and it has been investigated currently 29.
The engagement of the ligand (PD-L1 or PD-L2) and its receptor PD-1 in T cells shows downregulation of TCR, made them nonresponsive for T cells 24. The expression of PD-L1or PD-L2 is what some cancer cells do to avoid the immune system, to contrasts, this is necessary to blockage the interaction between PD-1 and these ligands 30,31. Nivolumab and Pembrolizumab are a humanized monoclonal antibody of IgG4 that alter the engagement between PD-1. In the case of Nivolumab blocks the interaction with the ligands PD-L1 and PD-L2 and Pembrolizumab with PD-L1 26,32.
Structure of nivolumab
The binding interaction between the crystal structure of nivolumab (PD – 1) and its binding section (PD – L1) suggest a competitive binding caused by steric clash to abrogating caused by the interaction 33. The steric clash of the binding interaction of protein is the result of atomic overlapping caused by the repulsing binding of the Van der Waals 34. In the case of nivolumab structure, the b-sheet of the interaction of PD – 1/ PD – L1 is dominated by N – loop. The variable loop (VL) chain interact on the surface overlapping the surface with PD – L1 33. As a result of this interaction, the complex PD – 1 / PD – L1 result of having a strong interaction due to the formation of new binding formation.
One fact of the interaction of nivolumab with its receptors (PD – L1) is the presence of glycosylation protein as an important role in the post-translational modification, important clue for any biological process, as it N- loop. Which is independent of nivolumab interaction, that implies a branch of tumor cell studies, considering that the expression of PD – 1 in tumor cells also include glycan modifications. The importance of maintaining the protein glycosylation formed in the nivolumab complex is that the alteration of these patterns could result in an incomplete synthesis and neo – synthesis processes in tumor cells. On the other hand, the N – loop dominated binding in nivolumab indicates the flexibility if N – a loop of PD – 1, open new ruts of researches on PD – 1/ PD – L1 blockade antibody design 33.
The interaction of the nivolumab with its corresponding receptor is shown in the type and number of receptors involved. In figure 1 are shown the formation of hydrogen bonds between nivolumab and PD – 1 in red and van der Waal interaction in pink, with a total of residues involved in bridge formation of 18 residues. In the same way, figure 1 show residues involved in the interaction of nivolumab and PD – 1; green for the heavy chain and orange for the light chain, having a total of 15 residues in total. 29
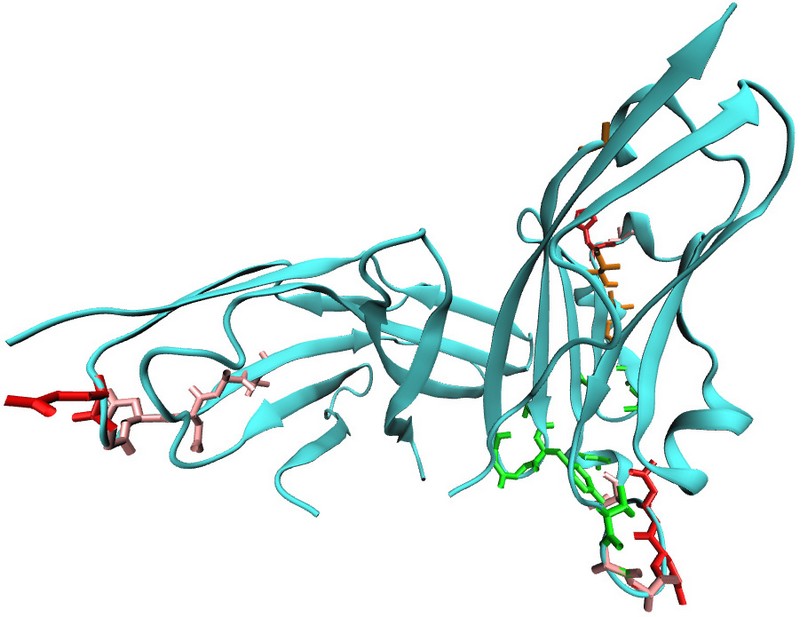
Figure 1. Initial state of the immunoglobulin nivolumab. Representation of the antibodies nivolumab (PDB:4ZQK). The initial conformation state of the immunoglobulin shows the amino acid of the heavy and light chain.
Structure of Pembrolizumab
The crystallized structure of the immunoglobulin IG4 pembrolizumab presents particular properties of this subclass, like as immune checkpoint inhibitory activity 26. This ability allows it to inhibit the interaction among the programmed death cell death protein (PD -1) and T-cell 28. Nowadays the interaction of immune checkpoints and its complexes, like as ligands antibodies and small molecules is deeply study as targeting therapy of cancer 27.
The study of molecular identification or the crystal structure of cancer antigens is the focus of some researches due to the new approach for effectives therapies. Nowadays is currently study the PD1 receptor in cancer immunotherapy 28.
The complex interaction of PD – 1 pembrolizumab have a complex crystallized structure of 1.2 Å 29 with an asymmetrical Y shape and symmetrical high regions (26). The complete structure suggests the mechanism in which the antibody block interaction of PD – 1/PD – L1 is given through outcompeting; in other words, it’s more successful than the competitor 28. The epitope region of the pembrolizumab with PD – 1, such as other type of antibodies, is conformed of discontinues segments. Furthermore, the binding of the complex PD – 1/pembrolizumab produce a conformational change in the BC loop and the FG loop, making the binging with PD – L1 incompatible 29.
The complex interaction of the pembrolizumab with its corresponding PD – 1 is shown in the type and number of receptors involved. This interaction has more variety of bond formation and residues involved than nivolumab, showing more stability of interaction. In figure 1 are shown the bond formation between pembrolizumab and PD – 1 with hydrogen bond in red, van der Waal interaction in pink, water mediated in yellow and salt bridges in grey; with a total of residues involved in bridge formation of 33 residues. In the same way, figure 2 show residues involve in the interaction of pembrolizumab and PD – 1; green for the heavy chain and orange for the light chain, having a total of 29 residues in total. 29
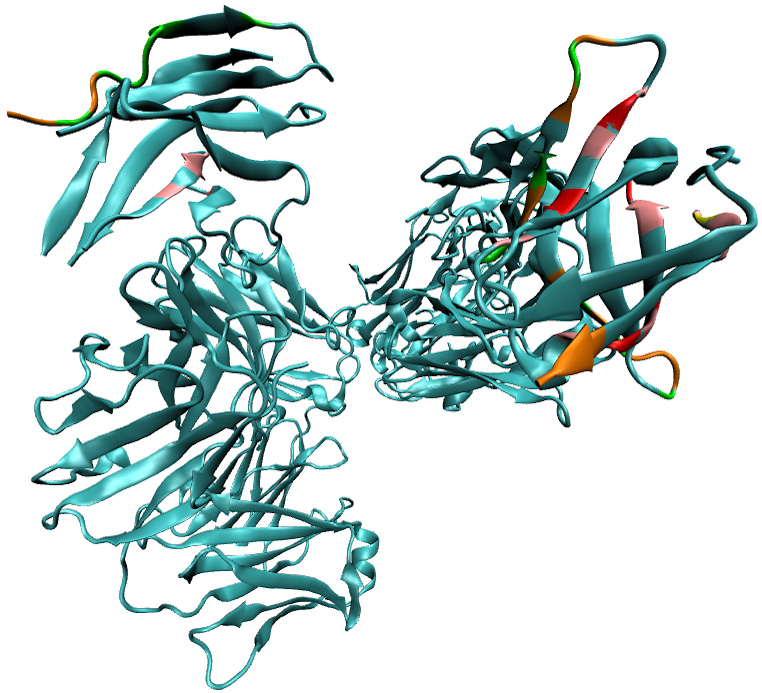
Figure 2: Initial state of the immunoglobulin pembrolizumab. Representation of the antibodies pembrolizumab (PDB:5JXE). The initial conformation state of the immunoglobulin shows the amino acid of the heavy and light chain.
Nivolumab and Pembrolizumab in lung cancer
Nivolumab and Pembrolizumab are currently being used in the treatment of Non-small Cell Lung cancer due to the great improvement that represents the use of presents in the treatment of cancer in comparison with other types of therapies. All these data are clearly shown in the clinical trials that had made with Nivolumab and Pembrolizumab 35. This review analyzes the clinical trials made with nivolumab or pembrolizumab vs chemotherapy. In addition to that this review also includes an analysis of a clinical trial in which nivolumab and pembrolizumab were compared directly.
Nivolumab and Pembrolizumab vs. platinum-based therapy
How it's better than other treatment
Several medicine proposals are available for researches to preprocess, named checkmate for nivolumab researches and keynote for pembrolizumab researches, with variable results. We aimed to compare different medicine for non-small cell lung cancer available for nivolumab and pembrolizumab and compare those results with available chemotherapy treatments.
The comparison results are resume in table 1. Where can be demonstrated that treatment with pembrolizumab (50% tumor cell expression) for NSCLC treatment have longer progression-free survival (PFS) and mean overlap survival (OS) compare with chemotherapy treatment (platinum-based).
In the other hand, not significant longer PSF and OS where show between nivolumab and chemotherapy treatment at 5% level expression- Table 1 is of current cancer treatment for NSCLC; (immune checkpoint blockades vs chemotherapy) by comparing the results on clinical trials.
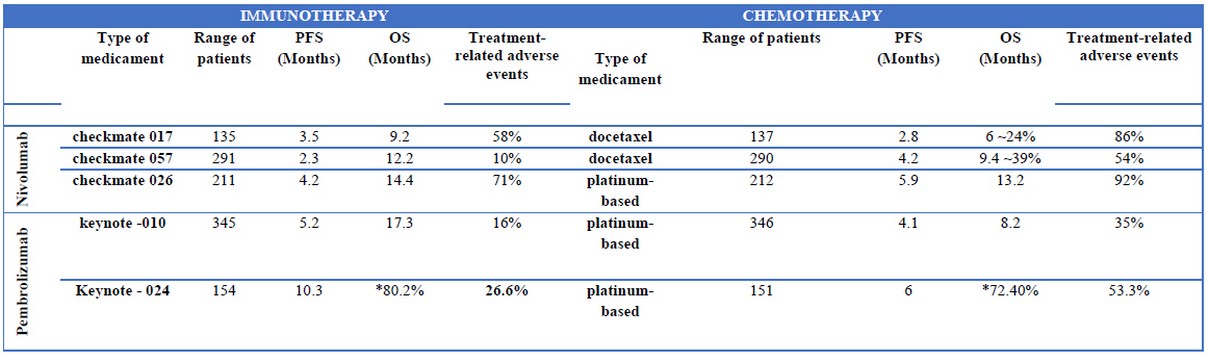
Tab 1: Comparison based on the rate of success of different treatment. The variation on the number of patients considered for each study is not taken as a major influence in the general comparison of the result of the clinical trials. The histology was also take in count. The number of death during the experiment was not taking in count due to the influence of diverse adverse effects implied of the medicament that may affect or influence on the development of cancer.
NDA = No Data Available
PFS = Median Progression Free Survival
OS = Median Overall Survival
*The median overall survival was not reached in both groups, so it was estimated the percentage of patients alive at six months.
The results of these trials clearly show that Pembrolizumab is better in the treatment of NSCLC because it increases the survival rates, adverse effects are less, and objective response is higher. Pembrolizumab has many benefits over chemotherapy and can be considered to treat advanced non-small cell lung cancer that has over 50% of the presence of PD-L1 in tumor cells.
Nivolumab and Pembrolizumab
The study present was an experiment with patients with advanced non-small cell lung cancer in stage IV, which 230 were treated with nivolumab and 41 with pembrolizumab to evaluated their secondary effects and their effectiveness. The differences in the number of patients treated with every drug are due to eligibility criteria. The drugs were administrated according to standard doses 3mg/kg every two weeks in nivolumab and 2mg/kg every three weeks in the case of pembrolizumab. The result of this experiment is summarized in Table 2 36.
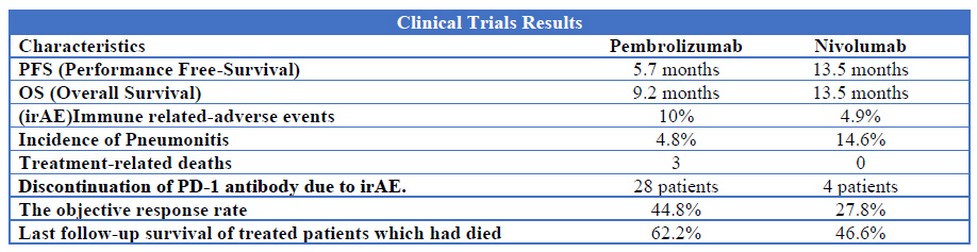
Table 2: Comparison of clinical between Pembrolizumab and Nivolumab in which the patients have NSCLC stage IV and were assigned to each group.
The results showed better results for pembrolizumab than nivolumab, although these results are statistically limited due to the differences in the number of patients treated with each drug. In addition to that, there were some parameters to assign the patient to the treatment, so there exists some bias. There exist a wider range to patients that can be treated with Nivolumab than Pembrolizumab.
Another important aspect to take in consideration these treatments is the cost. In the case of Nivolumab the overall cost is $103,220 37, Pembrolizumab 160,000 and chemotherapy 73,000 38. Although a better measure is the incremental cost-effectiveness ratio (ICER) that denotes the necessary payment for an additional year for these treatments. The ICER for nivolumab is $117,857, for chemotherapy $185,802 and for pembrolizumab is $98,421 (34). As we can see, pembrolizumab has better cost-effectiveness for NSCLC than nivolumab although the cost of pembrolizumab is higher.
CONCLUSIONS
Pembrolizumab and Nivolumab had shown better results in the treatment of non- small cell lung cancer in comparison with chemotherapy. This could be because both drugs improve the capacity of the immune system to recognize and attack tumor cells. Nivolumab had less adverse effects than chemotherapy, although the general survival did not have significant differences. By the other side, Pembrolizumab shows better results in survival and adverse effects in comparison with chemotherapy. Pembrolizumab and Nivolumab are anti-PD-1 receptors, although there are some structural differences that in the clinical trial had shown better results for Pembrolizumab in patients with PD-L1 expression over 50%. Future research should include a direct comparison between both drugs with the same conditions and number of patients for both groups.
REFERENCES
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;
2. National Cancer Institute. Estadísticas del cáncer. 2018;20:1–5. Available from: https://www.cancer.gov/espanol/cancer/naturaleza/estadisticas
3. Perraso V. 10 Gráficos Para Entender El Grave Impacto Del Cáncer En El Mundo. Bbc. 2016;http://www.bbc.com/mundo/noticias/2016/02/160203_c.
4. World Health Organization. Cáncer [Internet]. Cáncer. 2018. Available from: http://www.who.int/es/news-room/fact-sheets/detail/cancer
5. Ministerio de Salud Publica del Ecuador. Estrategia nacional para la atención integral del cáncer en el Ecuador [Internet]. 2017. Available from: https://aplicaciones.msp.gob.ec/salud/archivosdigitales/documentosDirecciones/dnn/archivos/ac_0059_2017.pdf
6. González S. Cáncer de pulmón, uno de los más agresivos en Ecuador. Diario La Hora [Internet]. 2017;1–3. Available from: https://lahora.com.ec/noticia/1102046320/cc3a1ncer-de-pulmc3b3n-uno-de-los-mc3a1s-agresivos-en-ecuador
7. Cordero FC, Ayala PC, Maldonado JY, Montenegro WT. Trends in cancer incidence and mortality over three decades in Quito-Ecuador. Colomb Med. 2018;
8. FDA. Pembrolizumab ( Keytruda ) 5-10-2017 [Internet]. 2017. p. 10–1. Available from: https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm558048.htm
9. Sundar R, Cho BC, Brahmer JR, Soo RA. Nivolumab in NSCLC: Latest evidence and clinical potential. Therapeutic Advances in Medical Oncology. 2015.
10. FDA. FDA Approves Pembrolizumab in Combination With Chemotherapy for First-Line Treatment of Metastatic Nonsquamous NSCLC [Internet]. 2018. p. 1–2. Available from: https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm624659.htm
11. Couzin-Frankel J. A cancer drug’s broad swipe. Science (80- ). 2017;358(6370):1520–1.
12. Khuder SA, Lally CA, Flannery JT, Calle EE, Flanders WD, Heath CW, et al. Effect of cigarette smoking on major histological types of lung cancer: a meta-analysis. Lung cancer [Internet]. 2001;31(2–3):139–48. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11165392
13. Zappa C, Mousa SA. Non-small cell lung cancer: current treatment and future advances. Transl Lung Cancer Res. 2016;
14. Kalemkerian GP. Small Cell Lung Cancer. Semin Respir Crit Care Med. 2016;37(5):783–96.
15. Gridelli C, Rossi A, Carbone DP, Guarize J, Karachaliou N, Mok T, et al. Non-small-cell lung cancer. Nat Rev Dis Prim. 2015;
16. Howington JA, Blum MG, Chang AC, Balekian AA, Murthy SC. Treatment of Stage I and II Non-small Cell Lung Cancer. Chest [Internet]. 2013 May 1;143(5):e278S-e313S. Available from: https://doi.org/10.1378/chest.12-2359
17. Ramalingam S, Belani C. Systemic Chemotherapy for Advanced Non-Small Cell Lung Cancer: Recent Advances and Future Directions. Oncologist [Internet]. 2008;13(Supplement 1):5–13. Available from: http://theoncologist.alphamedpress.org/cgi/doi/10.1634/theoncologist.13-S1-5
18. West H, Jin JO. Performance status in patients with cancer. JAMA Oncology. 2015.
19. Masters GA, Temin S, Azzoli CG, Giaccone G, Baker S, Brahmer JR, et al. Systemic Therapy for Stage IV Non–Small-Cell Lung Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol [Internet]. 2015;33(30):3488–515. Available from: https://doi.org/10.1200/JCO.2015.62.1342
20. Amini A, Yeh N, Gaspar LE, Kavanagh B, Karam SD. Stereotactic body radiation therapy (SBRT) for lung cancer patients previously treated with conventional radiotherapy: A review. Vol. 9, Radiation Oncology. 2014.
21. Schreiber RD, Old LJ, Smyth MJ. Cancer Immunoediting: Integrating Immunity’s Roles in Cancer Suppression and Promotion. Science (80- ) [Internet]. 2011 Mar 25;331(6024):1565 LP – 1570. Available from: http://science.sciencemag.org/content/331/6024/1565.abstract
22. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nature Reviews Cancer. 2012.
23. Mahoney KM, Freeman GJ, McDermott DF. The Next Immune-Checkpoint Inhibitors: PD-1/PD-L1 Blockade in Melanoma. Clin Ther [Internet]. 2015 Apr 1;37(4):764–82. Available from: https://doi.org/10.1016/j.clinthera.2015.02.018
24. Haanen JBAG, Robert C. Immune Checkpoint Inhibitors. In: Progress in Tumor Research [Internet]. 2015. p. 55–66. Available from: https://www.karger.com/DOI/10.1159/000437178
25. Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, et al. Pembrolizumab for the Treatment of Non–Small-Cell Lung Cancer. N Engl J Med [Internet]. 2015;372(21):2018–28. Available from: https://doi.org/10.1056/NEJMoa1501824
26. Scapin G, Yang X, Prosise WW, McCoy M, Reichert P, Johnston JM, et al. Structure of full-length human anti-PD1 therapeutic IgG4 antibody pembrolizumab. Nat Struct Mol Biol. 2015;
27. Zak KM, Grudnik P, Magiera K, Dömling A, Dubin G, Holak TA. Structural Biology of the Immune Checkpoint Receptor PD-1 and Its Ligands PD-L1/PD-L2. Structure [Internet]. 2017 Aug 1;25(8):1163–74. Available from: https://doi.org/10.1016/j.str.2017.06.011
28. Tavares ABMLA, Lima Neto JX, Fulco UL, Albuquerque EL. Inhibition of the checkpoint protein PD-1 by the therapeutic antibody pembrolizumab outlined by quantum chemistry. Sci Rep. 2018;
29. Lee JY, Lee HT, Shin W, Chae J, Choi J, Kim SH, et al. Structural basis of checkpoint blockade by monoclonal antibodies in cancer immunotherapy. Nat Commun. 2016;
30. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N Engl J Med [Internet]. 2016;375(19):1823–33. Available from: https://doi.org/10.1056/NEJMoa1606774
31. Ghiotto M, Gauthier L, Serriari N, Pastor S, Truneh A, Nunès JA, et al. PD-L1 and PD-L2 differ in their molecular mechanisms of interaction with PD-1. Int Immunol. 2010;
32. Robert C, Long G V., Brady B, Dutriaux C, Maio M, Mortier L, et al. Nivolumab in Previously Untreated Melanoma without BRAF Mutation. N Engl J Med. 2015;
33. Tan S, Zhang H, Chai Y, Song H, Tong Z, Wang Q, et al. An unexpected N-terminal loop in PD-1 dominates binding by nivolumab. Nat Commun. 2017;
34. Verma V, Sprave T, Haque W, Simone CB, Chang JY, Welsh JW, et al. A systematic review of the cost and cost-effectiveness studies of immune checkpoint inhibitors. J Immunother Cancer. 2018;
35. Pabani A, Butts CA. The current landscape of immunotherapy for the treatment of metastatic non-small-cell lung cancer. Curr Oncol. 2018 Jun;25(Suppl 1): S94–102.
36. Ksienski D, Wai ES, Croteau N, Fiorino L, Brooks E, Poonja Z, et al. Efficacy of Nivolumab and Pembrolizumab in Patients With Advanced Non–Small-Cell Lung Cancer Needing Treatment Interruption Because of Adverse Events: A Retrospective Multicenter Analysis. Clin Lung Cancer [Internet]. 2018; Available from https://doi.org/10.1016/j.cllc.2018.09.005
37. Andrews A. Treating with Checkpoint Inhibitors-Figure $1 Million per Patient. Am Heal drug benefits. 2015;
38. Georgieva M, da Silveira Nogueira Lima JP, Aguiar Jr. P, de Lima Lopes Jr. G, Haaland B. Cost-effectiveness of pembrolizumab as first-line therapy for advanced non-small cell lung cancer. Lung Cancer [Internet]. 2018 Oct 1;124:248–54. Available from: https://doi.org/10.1016/j.lungcan.2018.08.018
Received:14 May 2019
Accepted:15 July 2019
Camila Lissett Velastegui Gamboa and Dayanara Lissette Yánez Arcos
Yachay University of Experimental Technological Research. Ecuador
Dayanara Lissette Yánez Arcos
https://orcid.org/0000-0003-4823-1126
Camila Lissett Velasteguí Gamboa
https://orchid.org/0000-0002-0340-6247
Corresponding author: [email protected]