2023.08.01.57
Files > Volume 8 > Vol 8 No 1 2023
Characterization of alcohol levels in autopsies carried out by Forensic Medicine (Honduras) during December 2022 and January 2023

Ismael Raudales1, Josué Pineda1, José Isaac Zablah2*, Antonio García Loureiro3, Yolly Molina2, Marcio Madrid2, Carlos A. Agudelo2, and Jorge Alberto Valle-Reconco2
1 Dirección de Medicina Forense, Ministerio Público (Honduras); [email protected], [email protected]
2 Facultad de Ciencias Médicas, Universidad Nacional Autónoma de Honduras (UNAH); [email protected], [email protected], [email protected], [email protected], [email protected]
3 Departamento de Electrónica y Computación, Universidad Santiago de Compostela, España; [email protected]
* Correspondencia: [email protected]; Tel.: (504) 2239-4292
Available from: http://dx.doi.org/10.21931/RB/2023.08.01.57
ABSTRACT
To determine the existing relationship between ethanol levels in biological fluids, such as blood and urine, and their correlation with causes of death in corpses admitted to the forensic medicine autopsy service in Honduras. The gas chromatography method was employed to determine the concentration of ethyl alcohol. After a statistical analysis using measures of central tendency, it was found that the urine sample presented a median of 227.30mg/dL, while in the blood, it was 276.86mg/dL. After some distribution tests and correlation, it was determined that higher alcohol concentrations influence the "ACCIDENTAL" cause of death, with values of median alcohol concentration of 228.56mg/dL in blood and 277.44 mg/dL in urine. Still, the most frequent cause of death was "HOMICIDE", which differs in the age of the subjects and their ethanol concentration, with values of median alcohol concentration of 227.20mg/dL in blood and 276.86mg/dL in urine; similarities of median indicates that both samples are related or share a standard feature. Subsequent statistical tests showed that blood concentration values are more representative than urine values since the latter represents the final metabolic stage of alcohol in the body and exhibits more excellent dispersion. The average age of the individuals analyzed was 33 years old. However, it should be noted that individuals involved in "ACCIDENTAL" causes of death were in the lower age range corresponding to the so-called young adults.
Keywords: Forensic sciences; blood alcohol concentration; autopsy; alcohol in urine
INTRODUCTION
Alcohol consumption is associated with crime, a topic of interest in public health. Multiple studies have determined that alcohol consumption increases an individual's likelihood of committing homicides and other violent crimes. Although this relationship has been extensively investigated, there are still challenges in identifying the factors contributing to this association and in implementing effective policies and strategies to prevent excessive alcohol consumption and thereby reduce the incidence of alcohol-related homicides1-3.
Forensic medicine services perform autopsies to investigate the causes of death in various countries. As part of the laboratory analysis protocol, an analysis of alcohol levels in the blood, urine, or vitreous humor is included, whichever is available, and the sample is reliable for research purposes. Care is taken to control environmental factors, safeguarding and adequately using controls so that the data obtained is reliable4.
As studies are conducted with corpses, these samples must be processed quickly to avoid spurious or inaccurate results. Therefore, an uncertainty value is used in the analysis to indicate how reliable the results of the alcohol analyses in various biological fluids are. According to statistics, alcohol consumption is more frequent in economically active young adults, usually occurring at night, on weekends, and especially during festive seasons5.
Internationally, it is known that there is a relationship between alcohol consumption and violent death. In Norway, in 2013, taking data from autopsies over fifteen years, it was found that alcohol levels in the blood of victims and perpetrators of homicides were present in more than half of the cases, significantly higher in the perpetrators6-7. In Australia, a study was carried out for five years on autopsies conducted for violent causes. It was found that alcohol consumption was present in more than half of the cases, with the peculiarity that the victims had higher levels of alcohol in their blood than the general population. This study, published in 2019, introduced the combination of alcohol with drugs of abuse8.
The age distribution of alcohol-related deaths over the last decade may vary depending on the region and country9. However, some studies suggest a tendency for alcohol-related violent deaths to affect young and middle-aged adults mainly. But there is a greater tendency for men to be affected by this cause than women, with an average age of deaths attributable to alcohol at around 49 years10-11. Another study published in 2016 analyzed alcohol-related mortality in Europe. The study found that most alcohol-related deaths occurred in people between 40 and 59 years old, followed by those between 60 and 79. Alcohol-related deaths disproportionately affect men12.
Globally, alcohol is directly related to multiple factors in which consumers participate in simple homicides, murders, and traffic accidents. In the case of suicides, they are typically combined with drug abuse such as benzodiazepines, cocaine, etc. In this study, the relationship between alcohol consumption and causes of death of corpses entered the Forensic Medicine autopsy service in Honduras is considered. December 2022 and January 2023 have been selected as they coincide with dates of higher alcohol intake due to seasonal holidays, sports events, and graduations.
The data from this research has been analyzed using descriptive statistics. Still, correlation and distribution tests have been used to describe ethanol values in blood and urine obtained by gas chromatography. The conclusions obtained from the statistically significant values, especially related to the causes of death for "HOMICIDE" and "ACCIDENTAL", considering the variables of ethanol concentration and age, will be found at the end.
MATERIALS AND METHODS
The data used in this article comes from autopsies performed by the Public Ministry in Tegucigalpa, Honduras, from December 2022 to January 2023; this sample is composed of a total of 45 bodies, in which a concentration of ethanol in blood and urine was presented in the subjects under study. All autopsies where ethanol was not detected were excluded. It is essential to mention that according to current legal regulations and approved procedures, forensic medical services perform mandatory alcohol testing in all autopsies that enter due to violent death.
Gas chromatography is used to determine the concentration of ethanol in blood and urine. This process requires following the conditions established by protocols for these analyses, and then separation is performed based on the chemical and physical properties of the sample13. Ethanol is detected by sensors that provide a quantitative reading of its concentration present in the object of study. A cross-sectional study design has been used, as information has been collected on the concentration of alcohol at the time of autopsy. An Agilent 7809A gas chromatograph with dual flame ionization detectors (GC-FID/FID) is used for measuring ethanol concentration.
No qualitative test is utilized in the forensic medicine service since the result must be subjected directly to a quantitative analysis, given its legal value. One cannot rely on any method that might provide a false positive or false negative, as decisions will be made based on these data, which will surely affect the freedom of one or several individuals related to the cause of death. The Conway method was abandoned many years ago and replaced with the double detector FID test to provide two analyses in one. All laboratories comply with ISO 17025 standards.
A standard curve is generated to determine the ethanol concentration using a mixture of substances such as ethanol, methanol, acetone, and n-propanol, which are brought to volume with isopropanol serving as the internal standard. Blood and urine samples are prepared with internal standards (in this case, isopropanol), enabling the detection and quantification of any of the aforementioned substances. A concentration of 10 mg/dL of ethanol in any sample is sufficient to indicate alcohol consumption, whereas lower concentrations are deemed negative.
These substances are crucial because isopropanol can sometimes be a product of decomposition in the body. Acetone is present when ethanol metabolism is incomplete, and individuals may also use perfumes, homemade disinfectants, and other products instead of alcoholic beverages. Methanol is used in laboratories to determine whether alcohol consumption may be due to poorly distilled or adulterated alcohol, which is more common in cases of multiple intoxications. It is worth noting that gas chromatography is used to determine the retention times of the substances under investigation, which is obtained by calculating the area under the curve of the peaks shown as results in this method.
The ethanol concentration in blood and urine can be used to determine the level of alcohol in a person's body. However, the relationship between the concentration of alcohol in blood and urine is not linear and can be affected by various factors, such as absorption, distribution, metabolism, and previous elimination14.
Blood values are considered the most accurate measure of a person's alcohol level at a given moment since they reflect the amount in the bloodstream. Urine concentration can be used to determine alcohol in the elimination stage but does not provide an accurate measure of the level in the body due to being influenced by the amount of water present in the body and the time elapsed since the last alcohol intake. Whether in blood or urine, values are expressed in milligrams of ethanol per deciliter of blood (mg/dL)15-16.
RESULTS
Data from 45 autopsies have been collected, all of which have confirmed evidence through laboratory analysis of the presence of ethanol in blood and urine. Of these, 43 were male (95.55%), and t were female (4.45%). The causes of admission were 13 "ACCIDENTAL," 29 "HOMICIDE," and 3 "SUICIDE". These data exhibit statistical behavior described in Table 1.
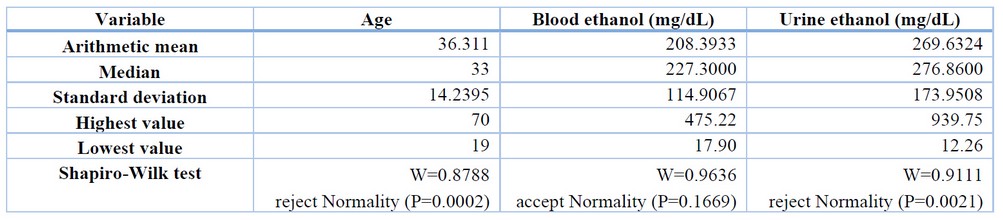
Table 1. Descriptive statistics of the sample (n=45). Only blood ethanol concentration shows a normal distribution behavior.
When performing a distribution test using the Shapiro-Wilk method, it was calculated that blood ethanol values showed a test statistic of 0.9636 with a p-value of 0.1669. For urine ethanol values, a test statistic of 0.9111 was obtained with a p-value of 0.0021, and finally, age had a value of 0.8788 with a p-value of 0.0002. The urine ethanol and age data do not follow a normal distribution but are skewed due to extreme values. Therefore, it is not possible to assume parametric assumptions in subsequent analyses. If statistical tests requiring normal distribution are performed, an alternative non-parametric approach should be sought, or the data should be transformed to meet the normality assumptions. Figure 1 graphically shows the ethanol concentration data with the normal distribution curve.
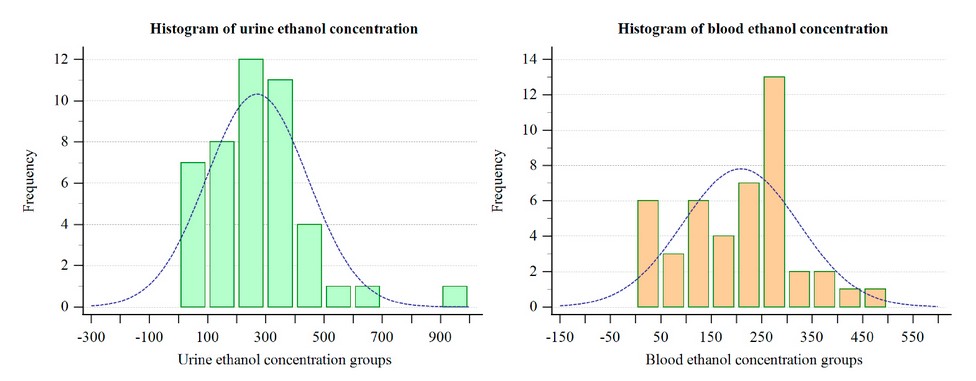
Figure 1. The ethanol concentration in urine has extreme data, unlike the concentration in blood, with more homogeneous data. The descriptive curve of the distribution of ethanol in urine is distorted.
Upon conducting the Mann-Whitney U test between the ethanol concentrations in blood and urine, a U value of 788 and a p-value of 0.0700 were obtained. Since the p-value is greater than 0.05, it indicates no significant differences between the concentrations. However, this conclusion is constrained by the sample size and representativeness of the original population.
When performing a bivariate analysis between blood and urine ethanol concentrations using the Pearson correlation test, a coefficient of 0.865 and a significance level of p-value < 0.0001 were obtained. This is interpreted as a moderate positive correlation between the two variables, suggesting that urine ethanol level is a good indicator of blood ethanol level in the sample used. Urine ethanol concentrations are, on average, higher than blood concentrations, but they show a more significant standard deviation, indicating that the values are more dispersed. For this study, blood ethanol was used because it showed less dispersed behavior and a normal distribution. Urine ethanol concentrations do not determine or correlate with a person's state because they are in the stage of bodily excretion. In contrast, blood values are altered more quickly after consuming alcoholic beverages.
There is no significant correlation between age and blood ethanol level (r=-0.07, p=0.66). An ANOVA analysis shows that blood ethanol level (F=8.91, p=0.0006) has a substantial effect on the cause of death ("ACCIDENTAL," "HOMICIDE," or "SUICIDE"). However, age does not significantly impact (F=0.11, p=0.74) the causes of death. Multiple comparisons were made using the Tukey HSD test to determine whether causes of death differ significantly in their blood ethanol levels. The results showed that levels are considerably higher in the "HOMICIDE" group than in the "ACCIDENTAL" group (mean difference = 147.10, p=0.006). To better characterize the data, Figure 2 shows their dispersion and trend.
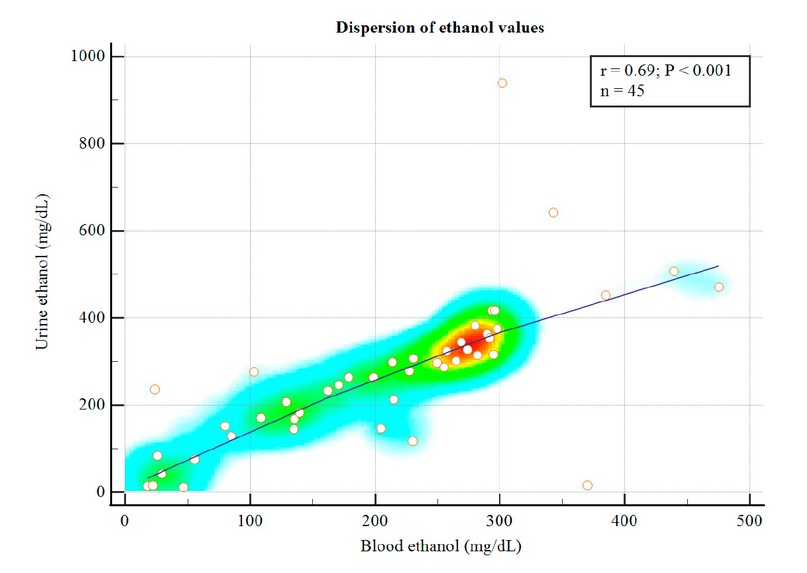
Figure 2. Dispersion of the data on the causes of death. Note the coloration of heat; in red, the highest concentration of data oscillates between 300mg/dL and 400mg/dL. Above the points is the trend line. The box shows the significant values of the statistical regression.
DISCUSSION
The results presented in this study show that blood alcohol levels are a crucial factor in determining the ability of a victim to operate machinery and make critical judgments. These findings highlight the importance of alcohol testing in legal proceedings, particularly in cases where the victim's state of mind is a crucial factor in determining guilt. Furthermore, the study also identifies age, sex, and race as significant factors in deciding blood ethanol concentration levels. This information could be helpful in legal cases where such demographic factors may impact the reliability of alcohol tests.
The study's finding that "HOMICIDE" is the most frequent cause of death for which a corpse arrives at the autopsy service is significant. The fact that this cause of death has higher blood alcohol concentrations than "ACCIDENTAL" causes implies that alcohol consumption plays a role in violent actions that lead to homicide. This finding highlights the importance of addressing the role of alcohol in violent crimes and its effects on social behavior. Studies indicate that alcohol is a more significant cause of accidents than acts of violence, a notable contrast with our findings17-18.
The results indicate that the behavior is similar to that reported by other authors19-20, with the main difference being the age range, which is more frequent among those under 28 years old in this sample. Although previous research has suggested other age ranges, 21-22, our study has provided further evidence. However, further studies are needed to confirm our findings and determine whether they are generalizable to other geographic regions.
The study's observation that most of the population under investigation is male is an important finding. The fact that females represent only a tiny proportion of the population studied with lower blood ethanol values suggests that gender may play a role in determining alcohol consumption and its effects. Future studies should explore this relationship further to provide insight into how gender-based differences in alcohol consumption may impact legal proceedings.
The sample has a strong male predominance and may not represent the general population, especially if an equal gender distribution is expected. It can also be inferred that any analysis of the sample and conclusions drawn from it may be biased toward the experiences and behaviors of men and may not apply to women or other populations with different gender distributions. Generally, it is essential to ensure that samples are large enough and representative to avoid incorrect or limited conclusions. That is why we only limit ourselves to indicating that it is a purely curious situation.
CONCLUSIONS
Additionally, blood alcohol levels determine whether a victim in an investigation was lucid, conscious, able to make critical judgments, and can operate automobiles, machinery, etc. Therefore, alcohol tests are a tool that helps the administration of justice, especially judges, to issue a guilty or not guilty verdict.
Due to the dispersion of ethanol concentrations in urine, it is not convenient to deduce blood alcohol values, as they are different stages of absorption, distribution, metabolism, and excretion (ADME). Therefore, they will always behave differently from each other. Other factors that influence ethanol concentration values are age, sex, and race."HOMICIDE" is the most frequent cause for which a corpse arrives at the autopsy service. Still, it has lower blood alcohol concentrations than the "ACCIDENTAL" cause. In the case of "SUICIDE," no analysis has been performed since this condition may be more associated with psychological factors than alcohol consumption. Another finding is that the population is almost entirely male. Only 4.45% correspond to females, with lower blood ethanol values of 50mg/dL. One died due to the "ACCIDENTAL" cause, and the other due to "HOMICIDE."
According to the descriptive statistical analysis performed, it was observed that the cause of "ACCIDENTAL" death is concentrated in young adults with blood ethanol values above 100mg/dL. In the case of "HOMICIDE" death, it is concentrated between the ages of 30 to 50 years, with blood ethanol values above 200mg/dL.
In general, it is concluded that alcohol does not directly affect "ACCIDENTAL" causes of death, as the age range of the subjects under study is in early adulthood. There is a growing public health problem due to the combined abuse of drugs and alcohol in this age range, as recorded in the forensic medicine service's database. This condition should be reviewed in future studies. On the other hand, the disinhibition effect generated by alcohol, combined with social breakdown situations, incites violent actions that end in "HOMICIDE" causes, hence the higher frequency of these.
Supplementary Materials: They have not been provided.
Author Contributions: Conceptualization, Ismael Raudales and Josue Pineda.; methodology, Yolly Molina and Marcio Madrid; validation, Ismael Raudales and Josue Pineda; formal analysis, Jorge Valle.; investigation, Yolly Molina.; data curation, Antonio Garcia Loureiro; writing—original draft preparation, Isaac Zablah; writing—review and editing, Carlos Agudelo; supervision, Jorge Valle; All authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Institutional Review Board Statement: Not applicable.
Informed Consent Statement: Not applicable.
Data Availability Statement: They have not been provided.
Acknowledgments: We thank the Directorate of Scientific, Humanistic, and Technological Research (DICIHT) for its support in the publication of this manuscript.
Conflicts of Interest: The authors declare no conflict of interest.
REFERENCES
1. James McKnight, A.; Langston, E. A.; Marques, P. R.; Tippetts, A. S. Estimating blood alcohol level from observable signs. Accid. Anal. Prev., 1997, 29(2), 247–255. DOI:10.1016/S0001-4575(96)00079-6
2. Ahlm, K.; Eriksson, A. Driver's alcohol and passenger's death in motor vehicle crashes. Traffic Inj Prev, 2006, 7(3), 219–223. DOI:10.1080/15389580600727846
3. Augsburger, M.; Donzé, N.; Ménétrey, A.; Brossard, C.; Sporkert, F.; Giroud, C.; Mangin, P. Concentration of drugs in the blood of suspected impaired drivers. Forensic Sci. Int., 2005, 153(1), 11–15. DOI: 10.1016/j.forsciint.2005.04.025
4. Dubowski, K. M. Alcohol determination in the clinical laboratory. Am J Clin Pathol, 1980, 74(5), 747–750. DOI:10.1093/ajcp/74.5.747
5. Nath, A.; Choudhari, S. G.; Dakhode, S. U.; Rannaware, A.; Gaidhane, A. M. Substance Abuse Amongst Adolescents: An Issue of Public Health Significance. Cureus, 2022, 14(11), e31193. DOI:10.7759/cureus.31193
6. Christophersen, A. S.; Gjerde, H.; Bjørneboe, A.; Sakshaug, J.; Mørland, J. Screening for drug use among Norwegian drivers suspected of driving under influence of alcohol or drugs. Forensic Sci. Int., 1990, 45(1–2), 5–14. DOI:10.1016/0379-0738(90)90216-l
7. Hjemsæter, A. J.; Bramness, J. G.; Drake, R.; Skeie, I.; Monsbakken, B.; Benth, J. Š.; Landheim, A. S. Mortality, cause of death and risk factors in patients with alcohol use disorder alone or poly-substance use disorders: a 19-year prospective cohort study. BMC Psych, 2019, 19(1), 101. DOI:10.1186/s12888-019-2077-8
8. Kõlves, K.; Draper, B. M.; Snowdon, J.; de Leo, D. Alcohol-use disorders and suicide: Results from a psychological autopsy study in Australia. Alcohol, 2017, 64, 29–35. DOI: 10.1016/j.alcohol.2017.05.005
9. Alpert, H. R.; Slater, M. E.; Yoon, Y.-H.; Chen, C. M.; Winstanley, N.; Esser, M. B. Alcohol Consumption and 15 Causes of Fatal Injuries: A Systematic Review and Meta-Analysis. Am J Prev Med, 2022, 63(2), 286–300. DOI: 10.1016/j.amepre.2022.03.025
10. Wilson, R. F.; Liu, G.; Lyons, B. H.; Petrosky, E.; Harrison, D. D.; Betz, C. J.; Blair, J. M. Surveillance for Violent Deaths - National Violent Death Reporting System, 42 States, the District of Columbia, and Puerto Rico, 2019. MMWR, 2022, 71(6), 1–40. DOI:10.15585/mmwr. ss7106a1
11. Volpicelli, J. R.; Menzies, P. Rethinking Unhealthy Alcohol Use in the United States: A Structured Review. Subst Abus Res Treat, 2022, 16, 11782218221111832. DOI:10.1177/11782218221111832
12. Jernigan, D.; Noel, J.; Landon, J.; Thornton, N.; Lobstein, T. Alcohol marketing and youth alcohol consumption: a systematic review of longitudinal studies published since 2008. Addiction, 2017, 112, 7–20. DOI:10.1111/add.13591
13. Wachełko, O.; Zawadzki, M.; Szpot, P. A novel procedure for stabilization of azide in biological samples and method for its determination (HS-GC-FID/FID). Sci Rep, 2021, 11(1), 15568. DOI:10.1038/s41598-021-95104-5
14. Biasotti, A. A.; Valentine, T. E. Blood alcohol concentration determined from urine samples as a practical equivalent or alternative to blood and breath alcohol tests. J Forensic Sci, 1985, 30(1), 194–207.
15. Kelly, A. T.; Mozayani, A. An Overview of Alcohol Testing and Interpretation in the 21st Century. J Pharm Pract, 2012, 25(1), 30–36. DOI:10.1177/0897190011431149
16. McKnight, A. J.; Langston, E. A.; McKnight, A. S.; Lange, J. E. Sobriety tests for low blood alcohol concentrations. Accid. Anal. Prev., 2002, 34(3), 305–311. DOI:10.1016/S0001-4575(01)00027-6
17. Sontate, K.V.; Rahim, K.M.; Naina, M.I.; Mohamed, R.M.P.; Shaikh, M.F.; Kamal, H.; Kumar, J. Alcohol, Aggression, and Violence: From Public Health to Neuroscience. Front. Psychol, 2021, 12, 699726. DOI:10.3389/fpsyg.2021.699726
18. Esser, M. B.; Leung, G.; Sherk, A.; Bohm, M. K.; Liu, Y.; Lu, H.; Naimi, T. S. Estimated deaths attributable to excessive alcohol use among US adults aged 20 to 64 years, 2015 to 2019. JAMA Netw Open, 2022 5(11), e2239485-e2239485 DOI:10.1001/jamanetworkopen.2022.39485
19. Alvarez, F.; Del Rio, M. Alcohol and driving. Lancet, 1996, 985(6), 347. DOI: 10.1016/s0140-6736(96)90139-7
20. Alvarez, F.; Del Rio, M. Alcohol y accidentes de tráfico: ¿Prevenir qué?. Trastornos Adictivos, 2001, 3(3), 172-180. DOI: 10.1016/S1575-0973(01)70030-X
21. Khiabani, H. Z.; Opdal, M. S.; Morland, J. R. Blood alcohol concentrations in apprehended drivers of cars and boats suspected to be impaired by the police. Traffic Inj Prev, 2008, 9(1), 31-36. DOI: 10.1080/15389580701737629
22. McLellan, B.; Vingilis, E.; Liban, C. Stoduto, G.; McMurtry, R.; Nelson, W. Blood alcohol testing of motor vehicle crash admissions at a regional trauma unit. J Trauma, 1990, 30(4), 418-421.
Received: January 15, 2023 / Accepted: February 25, 2023 / Published:15 March 2023
Citation: Raudales I, Pineda J, Zablah J I, García Loureiro A, Molina Y, Madrid M, Agudelo C A, Valle-Reconco J A. Characterization of alcohol levels in autopsies carried out by Forensic Medicine (Honduras) during December 2022 and January 2023. Revis Bionatura 2023;8 (1) 57. http://dx.doi.org/10.21931/RB/2023.08.01.57