2023.08.02.34
Files > Volume 8 > Vol 8 No 2 2023
Information and communication technologies (ICT) access indicators in the LGBTQ+ population with a high risk of contagion by acquired immunodeficiency virus (HIV) in Honduras

Salvador Diaz1,*, Mario Cooper4, Yolly Molina1, Isaac Zablah1, Antonio García Loureiro2, Carlos Agudelo-Santos1, Marcio Madrid1, Melania Madrid3, Jaffet Rodriguez3, Jorge Urmeneta1 and Jorge Valle Reconco1
1 Facultad de Ciencias Médicas, Universidad Nacional Autónoma de Honduras; [email protected], [email protected], [email protected] , [email protected], [email protected], [email protected], [email protected]
2 Departamento de Electrónica y Computación, Universidad Santiago de Compostela, España; [email protected]
3 Escuela de Microbiología, Facultad de Ciencias, Universidad Nacional Autónoma de Honduras; [email protected], [email protected]
4 Global Communities, Fondo Global, Honduras; [email protected]
* Correspondencia: [email protected]; Tel.: (504) 2239-4292
Available from: http://dx.doi.org/10.21931/RB/2023.08.02.34
ABSTRACT
In all societies, some populations are prioritized to be served by civil organizations and governments; access to technologies is typically left aside, especially in developing countries. The sample was for intentional contributions through the snowball method to reach 107 study participants. A survey-type instrument has been carried out where access, the use, and knowledge about convergent devices have been measured in a sample of individuals belonging to the lesbian, gay, bisexual, transgender, queer, and more (LGBTQ+) community. Basic statistics have been carried out to describe the frequencies of the sociodemographic variables and access to information and communication technologies (ICT). The LGBTQ+ community has access to convergent technologies, with a regular quality of service, with a preference for mobile devices and high daily use of them; there's an incongruence between income and spending on telecommunications services since it was perceived that this is a prioritized expense for all of them, even for those with the lowest economic income. The results of this study indicate that the LGBTQ+ community has significantly greater access to information technology and telecommunications services than the general population that hosts them; this study gives us a vision of how to offer technological solutions to prevent HIV in this community with a high incidence of this disease.
Keywords: ICT; Digital divide; LGBTQ+; Convergency
INTRODUCTION
The stigmatization and discrimination towards lesbian, gay, bisexual, transexual, queer, and more (LGBTQ+) people in Central American society can lead to the exclusion of this population, which translates into difficulties in accessing health information, HIV prevention, detection, and treatment services. This can lead to this population's exclusion and marginalization, which also causes legal and social barriers. Discriminatory and restrictive laws and policies descend directly on LGBTQ+ people, making access to HIV prevention and treatment services difficult, leading to an increased risk of infection and spreading the virus. This population, in turn, is subjected to violence and hate crimes, which become a constant concern in the region, leading to extremes of social exclusion1-4.
Information and communication technologies (ICT) have become essential enablers in almost all areas of human interest. They have allowed the evolution of humanity by incorporating hardware and software solutions at practically all levels, from entertainment, industry, and education to more complex aspects such as biomedicine, space science, and high-energy physics, among other fields. This has made it possible to make technologies more accessible to all humanity, each time getting closer to so-called universal access and service. The International Communications Union, an organization dependent on the United Nations, largely regulates these objectives and their standards and development.
The World Health Organization (WHO) has proposed Electronic Health (eHealth) as the support that the profitable and safe use of information and communication technologies offers to health and related areas, including health care services, health surveillance, and documentation, as well as health education, knowledge, and research. Consequently, with the possibilities offered by technological applications, there is a need to implement technologies adapted to the region and end users, defining objectives for each element of the applications and meeting the expectations of health professionals and patients when using health apps7-8.
When reviewing the databases available in the International Communication Union , it is observed that Honduras has yet to report complete information on the sector; the most relevant data is from more than fifteen years ago. While true global data is available, there is no way to know how these data are distributed among the population. Comisión Nacional de Telecomunicaciones (CONATEL) is the telecommunications regulatory body, it has a portal adapted to its own needs for statistical reports, focused more on inspection than on measurement tasks in the sector to determine the impact on society of the adoption of technologies. The National Institute of Statistics of Honduras (INE) conducts a Permanent Survey of Multi-Purpose Households, updated annually. Contains some global variables on access to technology and telecommunications; they are approached with a boolean perspective regarding access.9-12
The data for this research come from the project "HIV prevention through new information and communication technologies (ICT) in Honduras," which pursued the objective of being able to contribute to improving the access of key populations to complementary final services with a pleasant user experience that favors the prevention and diagnosis of HIV/AIDS, using convergent and ubiquitous technologies. At the time of this study, the scope of knowledge, attitudes, myths, and beliefs about using mobile applications and information and communication technologies for HIV prevention is unknown. Equally, there is a lack of data for analyzing costs, economic feasibility, and necessary resources to develop multi-device applications for the prevention and diagnosis of HIV in key populations, especially in the LGBTQ+ community.
In Central America this century, there is still an epidemic concentrated in specific key populations, such as men who have sex with men and transgender women. Prevalence rates are much higher in these groups than in the general population. The incidence rate per thousand inhabitants in Guatemala is 0.05, in Nicaragua 0.11, in El Salvador 0.13, in Panama 0.44, and in Honduras 0.07. Technology has played a vital role in the reduction, awareness, and detection of HIV in geographic regions, especially in the countries of North America and Europe. These strategies can be used in Honduras to reduce the number of new infections, focusing on crucial populations13-17.
In Honduras, the highest levels of resistance to antiretroviral therapy (ART) are fundamental problems in the success of treatment in HIV-infected patients. Resistance has been a growing problem in recent years; it is estimated through genotypic tests, which can help us end acquired resistance (in people who have not received treatment), Pre-ART resistance (in patients before receiving treatment), and transmitted resistance (develops once the person is under treatment). If the increase in resistance to therapy continues, it will become more challenging to treat the disease. Providing greater access to knowledge and availability of treatments is one way to reduce these conditions by allowing those infected to better adhere to treatment. Information and communication technologies can be how all this effort can be carried out for those affected. 18-19.
Increased vulnerability to HIV is often associated with legal and social factors, increasing exposure to risk situations and creating barriers to accessing effective, quality, and affordable HIV prevention, detection, and treatment services. Prioritizing key populations in the HIV response through appropriate interventions would most effectively address the epidemic and reduce new infections20.
To provide optimal care to people living with HIV, it is necessary to have quality information. Therefore, it is essential to ensure that the information obtained is stored securely and kept confidential to avoid stigmatization and discrimination of individuals and communities. This situation is strengthened and favored with the incorporation of ICTs, which allow interaction with people to be more agile and effective, reducing delays in information management and guaranteeing more excellent safety processes in its processing and other spheres; the linking of technologies in all health processes are decisive21-26.
There is no knowledge of the country's telecommunications access indicators, so measuring the variables already defined by the ITU as sector indicators is necessary to understand the use and opportunities of communication technologies—The information to reach the LGBTQ+ priority group.
Specifically, it is intended to analyze the necessary implementation processes in health and human resource skills, identifying the elements needed for successfully developing applications and information technologies to diagnose, treat, and prevent HIV. Likewise, with the access indicators, the capacity to determine the costs, economic feasibility, necessary resources, and conditions of implementing ICTs in terms of cost/benefit for the prevention, diagnosis, and management of HIV in key populations. For these checks, those already defined by ITU will be used in their known variables and ranges, which are the internationally accepted methods.
MATERIALS AND METHODS
A mixed approach was used since quantitative and qualitative elements were obtained through the questionnaire. The data obtained are primary since its main sources were collected directly from the target population. The type of research was non-experimental and cross-sectional since variables are not manipulated, and a single measurement is made over time. Still, the study has a descriptive scope because of the behavior on the use of the applications disclosed and information and communication technologies.
The instrument used was a semi-structured questionnaire with open and closed questions to collect data and thus answer the questions and objectives of the research. The study's target population was men who have sex with men (MSM), women who have sex with women (WSW), Garifuna, sex workers, HIV-positive people, women, and service providers from LGBTQ+ community organizations. The sample was by intentional quotas through the snowball method to reach the study participants in a way referred through the different organizations that supported the study. A total of 107 participants filled out the instruments used in this study.
The data obtained on access to ICT by the LGBTQ+ community is affected by the fact that not all organized groups can be accessed due to internal differences between them. This investigation was affected by being considered transgressive for some of them, so they preferred not to participate. This reflects the differences between the different associations.
The data analysis has been done through relative frequencies; with this, it will be possible to determine the technologies, costs, and most frequent uses by the LGBTQ+ community. These aid future decisions in prioritizing technologies and complementary end services to reach the end user of technology services more effectively.
The frequency analysis makes a count and each category's occurrence percentage. This allows you to visualize the data distribution and determine whether there are dominant categories or significant imbalances. This allows generating crossover tables to identify possible relationships or associations, providing us with a solid foundation to understand the composition and characteristics of a particular data set. By examining the frequencies, patterns, trends, and potential areas of interest for further investigation can be identified. This approach is beneficial in areas where a quantitative understanding of the distribution of categories within a population or sample of claim is required.
RESULTS
The sample consists of 107 people, according to their biological sex; it corresponds to 85 men and 22 women. Regarding the "sexual orientation" variable, most people identify as homosexual/gay (47%), followed by bisexual (19%), transgender (16%), transsexual (10%), lesbian (6%), pansexual, queer and transvestite (1%) each. The detail of this identification grouped by biological sex is detailed in Figure 1:
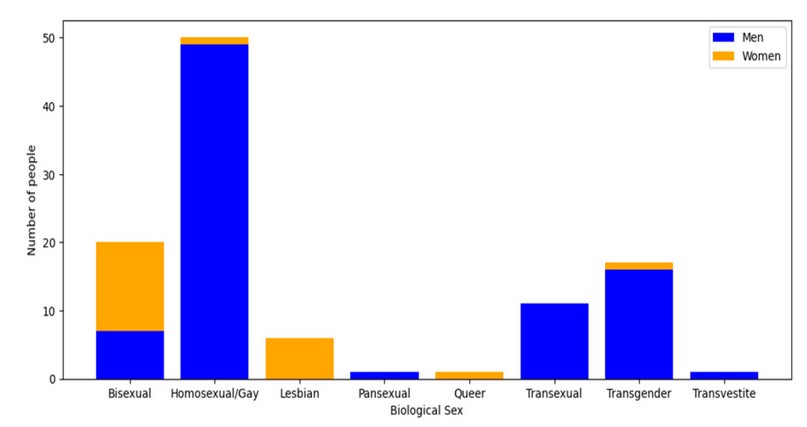
Figure 1. Biological sex grouped by sexual orientation
Regarding the age of all the participants, they have a mean of 31 years old, a standard deviation of 8.03 years, and a median of 30 years. The age range ranges from 18 to 61 years, with the most common age (mode) being 39 years old, which occurs in 8 individuals. When analyzing the frequency distribution, it is observed that the ages behave approximately normally, with a slight asymmetry to the left. Regarding the dispersion of generations, the coefficient of variation (Spearman's coefficient) is 0.26, which indicates a moderate variability between the ages of the individuals in the sample.
Regarding the maximum level of education reached, it is observed that most of the population has completed their secondary education (29%). The next largest group is the one with incomplete university education (24.3%), followed by the complete university (23.4%). The next group is the ones with the group of people with incomplete secondary education (10.3%), followed by people with complete primary education (9.3%). The most minor groups are people with incomplete primary education (2.8%) and people without education (0.9%).
Suppose the intersection of sexual orientation and education level is considered. In that case, it can be seen that the majority of people with completed college education identify as homosexual/gay (72%), while bisexual (12%) and transgender (12%) with the same proportion. Most people with completed elementary education identify as transgender (50%), bisexual (30%), and homosexual/gay (20%). People with completed high school are more evenly divided among different sexual orientations. The cumulative frequencies by sexual orientation are shown in Figure 2:
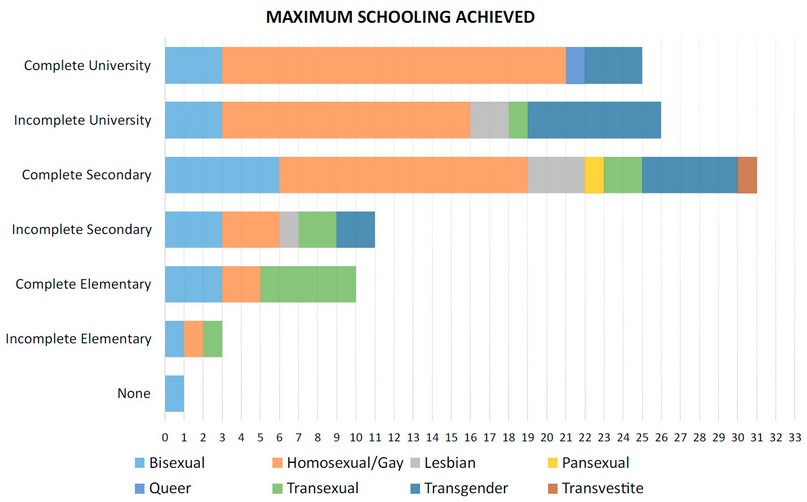
Figure 2. Schooling grouped by sexual orientation
Only 102 people in the sample have access to mobile services, and none consume services of the state telecommunications company. This service is available in the prepaid modality (this modality is known locally as recharges) (74%) and in postpaid (26%). Something notable is that in the set of postpaid users, when comparing their proportion compared to mobile users by sexual orientation, homosexuals/gays are the ones who use the most (60%), followed by transgender people (19 %) and transgender (19%), queer (2%). The other orientations do not have users in this mode.
It was observed that most homosexual/gay (60%) and bisexual (37%) users rated the mobile service as very good. Bisexual users had a more heterogeneous perception, with the excellent rating being the most frequent (42%) compared to their group as a whole, followed by regular (16%) and unstable (4%). Regarding the perception of lesbian users, there was a tendency to rate the mobile service as Good (40%) or very good (40%). In contrast, pansexual and queer users rated the service as good or average.
The operating system used in a mobile terminal, out of the total population, Android (90%) is the most common among all sexual orientations, followed by iOS (6%), exclusive to homosexuals/gays and lesbians, HarmonyOS (3%) used only by homosexuals/gay and transsexuals; Windows (1%) used by transgender people. Regarding having access to a tablet for personal or work use, 87% do not have access, and only 13% have that device, being the largest group of homosexuals/gay (43%), bisexuals (29%), transgender (21%), transsexuals (7%), the other orientations have no representation. The most used operating system is Android (86%), followed by and in the same proportion of Windows (7%) and iOS (7%) users.
Of the study population, 83% of those surveyed can use a personal computer, while 17% lack this ability. Of the respondents who can use a personal computer, 36% have a desktop computer, 50% have a laptop, and 14% have access to both devices. The operating system used by all respondents is of the Microsoft Windows type. The relative value of these variables grouped by sexual orientation is shown in Figure 3.
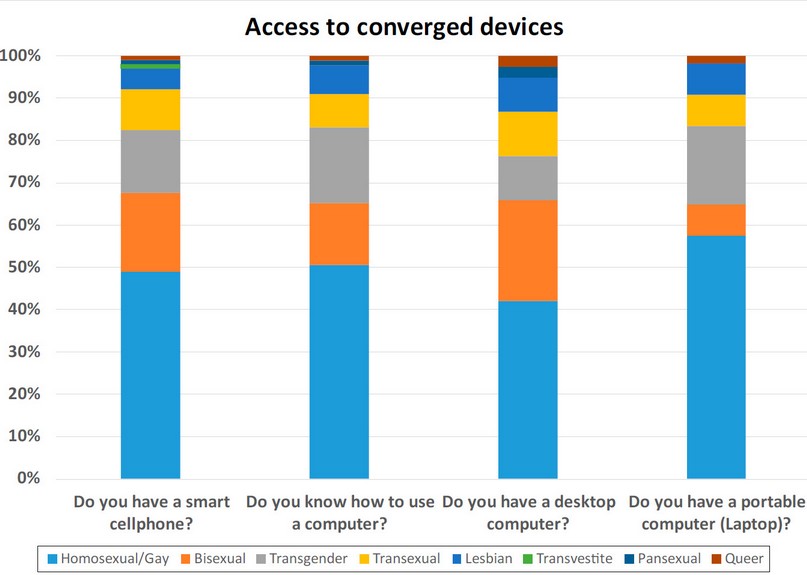
Figure 3. Cellphone, computer ability, and possession by sexual orientation
Regarding occupation, 43% of homosexuals/gays are dedicated to professional work, being classified the work as sanitary (17%), student (17%), commerce (15%), and informal sector (13%), where most of those identified with this orientation are concentrated. As for bisexuals, they are mainly dedicated to the informal sector (26%) and commerce (21%); transgenders are distributed across more occupations more evenly, with a higher concentration in the informal sector (29%), sanitary (14%), media (14%) and sex worker (14%). Transsexuals are grouped mostly in advocacy (27%), sex workers (27%), and the informal sector (18%). Lesbians are mainly from the sanitary segment (50%), followed by the informal sector (18%). The transvestites are dedicated to commerce, the pansexual in their entirety, the sanitary segment, and the queer to human rights. Figure 4 shows the percentage between different occupations.
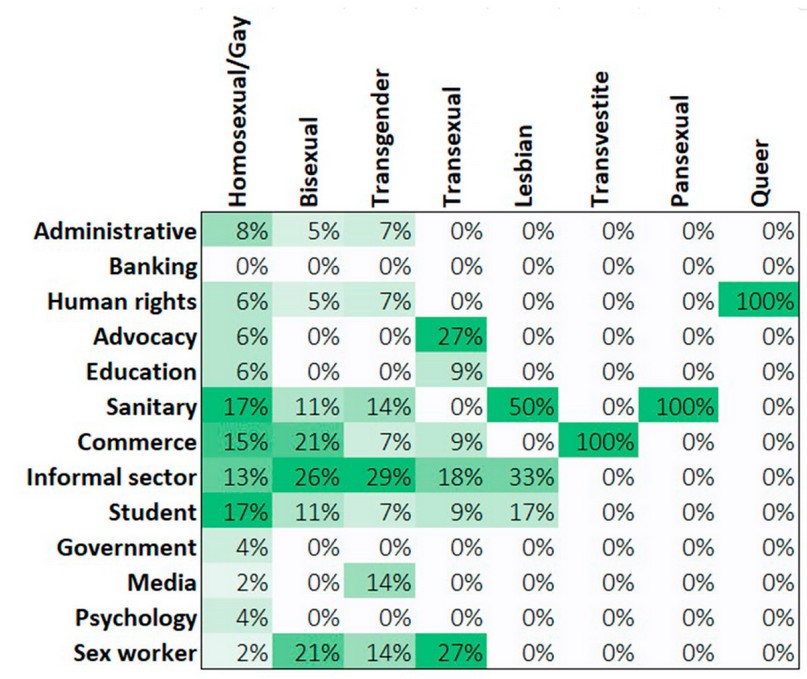
Figure 4. Occupation grouped by sexual orientation
The average income per respondent grouped by sexual orientation shows a very uneven behavior, so 52% of the respondents have incomes below the minimum wage established by labor laws in the country, in a clear situation of underemployment. The mode of income is the one that oscillates between USD$400 to USD$600, which 30% of the respondents have. Queers have the highest income (more than USD 800 per month), while transvestites are in a situation with the lowest income of all, barely surpassed by lesbians (46%), transsexuals (30%), and bisexuals (46%). The highest gains are distributed among homosexuals/gays (59%), Transgenders (77%), pansexuals (100%), and queers (100%), all of them above USD$400 per month.
The income is not directly proportional to the investment made in the prepaid mobile communications service, with a mode of an investment of more than USD$12 per month, which concentrates 47% of those surveyed. In comparison, 4% invest less than USD 2 a month. Grouped by sexual orientation, homosexuals/gay people invest mostly between US$12 to US$20 per month (38%), followed by US$8 to US$12 (25%) and more than US$20 (19%). Bisexuals (32%) spend between US$2 to US$6, followed by US$12 to US$20 (21%). Transgenders are distributed in various ranges of spending on mobile services, between USD$2 to USD$6 (20%), USD$6 to USD$8 (20%), USD$8 to USD$12 (20%), USD$12 to USD 20 (30%) and more than USD$20 (10%) in each range. Most transsexuals spend US$8 to US$12 (75%). Lesbians are equally distributed in four categories under $2 (25%), $2 to $6 (25%), $8 to $12 (25%), and over $20 (25%). All transvestites and pansexual consume more than USD$20 per month. The queers did not indicate consumption of mobile prepaid service. Detailed relative values can be viewed in Figure 5.
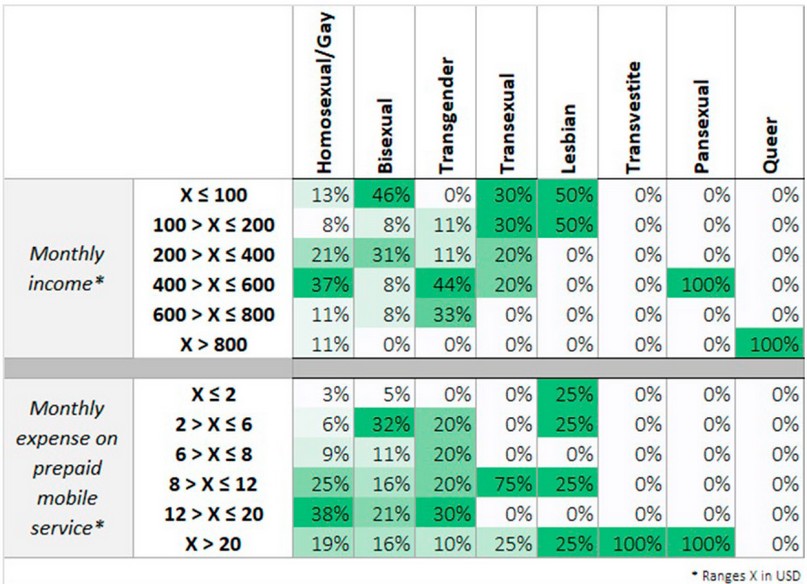
Figure 5. Monthly income and budget for mobile service grouped by sexual orientation
Access to technological devices that allow access to convergent networks, software, and complementary final applications is a disruptive component within the LGBTQ++ community. Regarding the number of hours of use of the devices, they indicate that they play a central role in their daily activities. Regarding the use of a computer, the trend among homosexuals/gay is to use it for more than four hours a day (41%), bisexuals for one hour or less a day (45%), and transgenders for between two and four hours (45%), transsexuals more than four hours (83%), the same as queer (100%). Transvestites and pansexuals do not have registered user information. Regarding the mobile, the trend is that all sexual orientations use this device more than four hours a day, applicable to 82% of homosexuals/gays, 72% of bisexuals, 93% of transgender people, 88% of transsexuals, 75% of lesbian, 100% transvestite and queer. Only pansexuals use it for less than or equal to one hour daily. Figure 6 shows the distribution of hours of use of converged devices.
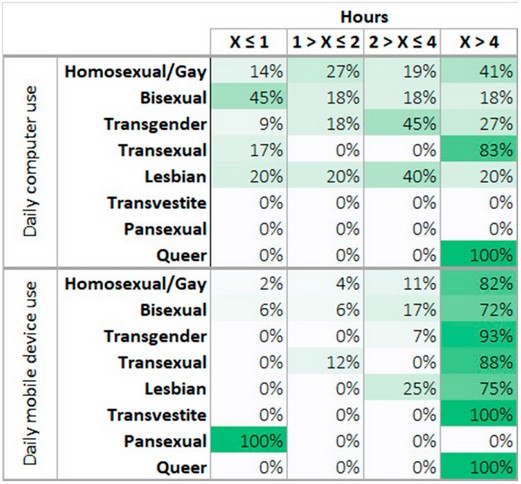
Figure 6. Daily usage time of mobile and computer grouped by sexual orientation
DISCUSSION
We find ourselves in the so-called information or knowledge society characterized because "organizations depend on the increasing use of intelligent information and information technology information to be competitive, and they are becoming organizations data-intensive 27.
Health promotion has been defined by the World Health Organization Health (2005) as "the process through which people achieve control over their health and its determinants, and therefore increase, improve your health." To achieve this objective, traditionally, the development of public policies aimed at improving different determinants of health, such as income level, housing, food, employment, and working conditions28.
The new information technologies make it possible to create and distribute content on the Internet quickly, efficiently, and cheaply. They can be very effective in promoting sexual health and the prevention of HIV and other STIs through direct communication with the users.
In this study, biological men identify with more sexual orientations, whereas women only identify as lesbian and bisexual. Two physical women in the sample selected an option as homosexual/gay (exclusive category for physical men) and one as queer. Still, it is the only data in that orientation. This behavior occurs for psychological, social, economic, and political reasons; cultural, ethical, legal, and religious, among others.
The highest concentration of respondents in the age range of 22 to 39 years old are economically active; this is an indicator that they do not have economic dependence on a third party, which is why it can be observed that there is greater diversity in terms of orientations sexual, a financial income allows to give the security to be able to accept their sexual reality without being affected by the perception of their relatives and close people.
75.9% of the sample has completed high school and university, indicating higher educational levels than those reported in Honduras in the Household Survey12. This condition is likely driving agendas to claim issues of interest in this specific social group. If the average age of those surveyed is 31 years, it is an indicator that this social group is well above the education average of the general population. 24.1% did not complete secondary education and are at low levels of training that do not empower them to integrate into the production gear and generate a form of economic discrimination. Homosexuals/gays are the sexual orientation with more individuals who have completed their university education; it indicates that they could more easily overcome bias and problems in educational institutions. Their main occupations are students and sanitary work.
The top five occupations among all sexual orientations are the informal sector (19%), the health sector (16%), commerce (14%), students (13%), and sex workers (10%). It is essential to highlight that it is one of the most weighted economic areas, such as the health sector, which represents the financial group with the highest income in the country, followed by merchants. The high number of individuals engaged in sexual services is notable but with highly variable income. The most significant number of people who identify as lesbian, bisexual, and transgender have the lowest income of the entire sample, with an amount below the minimum wage at the time of this study. Homosexuals/gays and transgender have higher incomes.
Regarding mobile services, 26% have the economic solvency and adequate credit record of having a postpaid line, while 74% use recharges. This is consistent when comparing the monthly income data. This is inversely proportional to the educational level; the majority (74%) have a mobile service based on recharges; Since it is cheaper to maintain and corresponds to people with a complete secondary education or less. As a curiosity, homosexuals/gays and lesbians mostly prefer the same telecommunications company, while the other groups prefer its competition.
Users whose sexual orientation is homosexual/gay, bisexual, or lesbian rate the mobile phone service as very good; however, the other orientations consider it good or average. This perception is consistent with their contract type since the postpaid service usually receives shared capacities and a lower quality of service. The mobile operating system Android (90%) is the most common among all sexual orientations, possibly because there is a greater variety in the price of these devices. The devices that use the iOS operating system (6%) are exclusive to homosexuals/gays and lesbians in the university studies group since this increases their purchasing power, allowing them to afford a higher-end terminal.
87% of the people surveyed do not have access to a tablet for personal or work use, and only 13% have this type of device, the largest group being homosexuals/gays (43%), reflecting higher incomes. All sexual orientations prefer mobile devices over personal computers, except queer. There is an increased adaptation of working life with the use of technologies; the service may be more significant within the LGBTQ+ community if we compare it with those presented in global details, as shown in the Permanent Survey of Multi-Purpose Households12.
The data found in this study is interesting since no previous studies refer to the use of technologies, specifically in the LGBTQ+ community. It is interesting since this population uses at least one electronic device and can use it to connect to social networks, commonly to find a partner. This could increase the possibility of irresponsible sexual encounters and contracting sexually transmitted diseases, including HIV29. Information and communication technologies (ICT) can help people with illnesses such as HIV regimen self-management their treatment and receive psychological support. For example, Gustavson et al. used one of the first sites of Web-based support for people living with HIV, known as the "Support System to Increase the Understanding Health" 30. In addition, CARE+ is a computerized counseling program to increase adherence to treatment antiretroviral and reduce the risk of transmission of HIV from people with this virus31. In patients who are in places with limited resources, the Cell Life project uses cell phones to monitor adherence and improve the management of HIV in patients who are on antiretroviral therapy 32.
The results indicate that using ICT to reach the LGBTQ+ community in Honduras to raise awareness, prevent, educate, inform, help, and treat HIV is viable. Similarly, these results can be extrapolated to reach this population for other purposes. Although the income of the majority is low, for them, it is a priority to remain in communication so that in the most challenging situations, a more personalized approach can be sought in the future for those individuals who are at risk of being marginalized, by providing them with access to technological means.
CONCLUSIONS
The scope of the research was mixed since quantitative and qualitative data were obtained through the instruments. These data suggest a relationship between sexual orientation and education level, although more data would be needed to confirm this relationship. However, these results can help formulate public policies and education and training programs that consider the diversity of the population in terms of sexual orientation and level of education attained.
The results indicate that sexual orientation can influence the perception of mobile service quality and that further research is needed on this topic to understand better the factors that influence the satisfaction of mobile service users. In this case, the data obtained from people who identify themselves as transvestites should be of particular attention to public policies; since these people are behind in educational and economic matters, they are likely a population subjected to exploitation and discrimination.
The LGBTQ+ community has a high degree of access to information technologies; they prefer mobile services and devices. They spend more than four hours a day using it. Therefore, any approach to people who identify sexually in non-traditional ways must consider converging technologies. The data indicates that they have more access and have a lower digital dividend when compared to the general population.
ICT is an essential tool for intervention in the LGBTQ+ population; until the moment of this study, it has not been adequately used for this purpose. The results indicated that this population uses ubiquitous technology based on mobile phones and complementary final services, allowing them to interact personally and anonymously, avoiding stigmatization and rejection.
The organizations that work with these populations and the public health services have an opportunity to advance even more in the fight and prevention of HIV in these populations; the same can be used to reach the people in general. Developing specific applications with electronic health services can help reduce the incidence of sexually transmitted diseases, including HIV and other pathologies in general. This can be framed in the country's health and human development programs.
Supplementary Materials: They have not been provided.
Author Contributions: Conceptualization, Mario Cooper and Salvador Diaz.; methodology, Yolly Molina and Marcio Madrid; validation, Melania Madrid and Jaffet Rodriguez; formal analysis, Jorge Valle-Reconco; investigation, Yolly Molina.; data curation, Antonio Garcia Loureiro; writing—original draft preparation, Isaac Zablah; writing—review and editing, Carlos Agudelo-Santos; supervision, Salvador Diaz and Jorge Urmeneta; All authors have read and agreed to the published version of the manuscript.
Funding: This research was funded by FONDO GLOBAL through Global Communities.
Institutional Review Board Statement: Not applicable.
Informed Consent Statement: Not applicable.
Data Availability Statement: Not applicable.
Acknowledgments: We thank the Directorate of the CEPROSAF, ASONAPVSIDAH, Liga de la Lactancia Materna de Honduras, and KUKULKAN Association for their support in getting the data used in the publication of this manuscript.
Conflicts of Interest: The authors declare no conflict of interest.
REFERENCES
1. Winton A. 'I've got to go somewhere': Queer Displacement in Northern Central America and Southern Mexico. In: LGBTI Asylum Seekers and Refugees from a Legal and Political Perspective. Cham: Springer International Publishing; 2019. p. 95–113.
2. Cupples J, Palomino-Schalscha M, Prieto M, editores. The Routledge Handbook of Latin American Development. London ; New York : Routledge, 2019.: Routledge; 2018.
3. Hobson EK. LGBTQ politics in America since 1945. Oxford University Press; 2017.
4. Wheeler DA. Availability of HIV care in Central America. JAMA. 2001, 286(7):853. DOI: 10.1001/jama.286.7.853
5. Alperin H, Mariscal J. Digital Poverty: Latin American and Caribbean perspectives. Practical Action Publishing; UK, 2007.
6. Codding GA Jr. Evolution of the ITU. Tel Pol. 1991, 15(4):271–85. DOI: 10.1016/0308-5961(91)90050-l
7. World Health Organization. Building foundations for ehealth: Progress of member states : Report of the WHO global observatory for EHealth. World Health Organization, Ginebra, Suiza, 2006.
8. Hanafizadeh MR, Saghaei A, Hanafizadeh P. An index for cross-country analysis of ICT infrastructure and access. Tel Pol. 2009, 33(7):385–405. DOI: 10.1016/j.telpol.2009.03.008
9. World Telecommunication/ICT Indicators Database. Available online: https://www.itu.int/en/ITU-D/Statistics/Pages/publications/wtid.aspx (accessed on 29-Jan-2023)
10. The world's richest source of ICT statistics and regulatory information. Available online: https://datahub.itu.int/ (Accessed on 29-Jan-2023)
11. Conatel – Comision Nacional de Telecomunicaciones. Available online: https://www.conatel.gob.hn/ (Accessed on 29-Jan-2023)
12. ENCUESTA PERMANENTE DE HOGARES DE PROPÓSITOS MÚLTIPLES – INE (2022). Available online: https://ine.gob.hn/V3/ephpm/ (Accessed on 23-Jan-2023)
13. Estrada M JH. Modelos DE prevención en la Lucha Contra El VIH/SIDA. Acta Bioeth. 2006, 12(1). DOI: 10.4067/s1726-569x2006000100013
14. John Harold E. La infeccion por VIH/SIDA entre hombres que tiene sexo con hombres (HSH) en America Latina. Rev Fac Nac de Salud Publica. 2004, 22(1):107–20.
15. Cáceres CF. Cad Saude Publica. 2004, 20(6):1468–85. DOI: 10.1590/s0102-311x2004000600004
16. Noar SM, Black HG, Pierce LB. Efficacy of computer technology-based HIV prevention interventions: a meta-analysis. AIDS. 2009, 23(1):107–15. DOI: 10.1097/QAD.0b013e32831c5500
17. Neumann MS, Sogolow ED. Replicating effective programs: HIV/AIDS prevention technology transfer. AIDS Educ Prev. 2000;12(5 Suppl):35–48.
18. Parham L, de Rivera IL, Murillo W, Naver L, Largaespada N, Albert J, et al. Short communication: high prevalence of drug resistance in HIV type 1-infected children born in Honduras and Belize 2001 to 2004. AIDS Res Hum Retroviruses. 2011, 27(10):1055–9. DOI: 10.1089/AID.2010.0289
19. Avila-Ríos S, García-Morales C, Tapia-Trejo D, Meza RI, Nuñez SM, Parham L, et al. HIV drug resistance surveillance in Honduras after a decade of widespread antiretroviral therapy. PLoS One. 2015, 10(11):e0142604. DOI: 10.1371/journal.pone.0142604
20. Turner B. Honduras. In: The Statesman's Yearbook. Palgrave Macmillan, UK; 2005. p. 785–9.
21. Duggal M, Chakrapani V, Liberti L, Satyanarayna V, Varghese M, Singh P, et al. Acceptability of mobile phone-based nurse-delivered counseling intervention to improve HIV treatment adherence and self-care behaviors among HIV-positive women in India. AIDS Patient Care STDS. 2018, 32(9):349–59. DOI: 10.1089/apc.2017.0315
22. Fisher CB, Bragard E, Bloom R. Ethical considerations in HIV eHealth intervention research: Implications for informational risk in recruitment, data maintenance, and consent procedures. Curr HIV/AIDS Rep. 2020, 17(3):180–9. DOI: 10.1007/s11904-020-00489-z
23. Paperny DM. Computerized health assessment and education for adolescent HIV and STD prevention in health care settings and schools. Health Educ Behav. 1997, 24(1):54–70. DOI: 10.1177/109019819702400107
24. Tomnay JE, Pitts MK, Fairley CK. New technology and partner notification--why aren't we using them?. Int J STD AIDS. 2005, 16(1):19–22. DOI: 10.1258/0956462052932700
25. Flicker S, Goldberg E, Read S, Veinot T, McClelland A, Saulnier P, et al. HIV-positive youth's perspectives on the Internet and e-health. J Med Internet Res. 2004, 6(3):e32. DOI: 10.2196/jmir.6.3.e32
26. León A, Cáceres C, Fernández E, Chausa P, Martin M, Codina C, et al. A new multidisciplinary home care telemedicine system to monitor stable chronic human immunodeficiency virus-infected patients: a randomized study. PLoS One. 2011, 6(1):e14515. DOI: 10.1371/journal.pone.0014515
27. Ministerio de Sanidad PS e. I-G de E. Prevencion del VIH a traves de las nuevas tecnologias de la informacion y la comunicacion. 2011. Available online: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/docs/VIH_TIC.pdf
(Accessed on 23-Jan-2023)
28. World Health Organization. The Bangkok Charter for Health Promotion in a globalised world. Health promotion journal of Australia: official journal of Australian Association of Health Promotion Professionals. 2005;16(3).
29. Sumter S., Vandenbosch L., Ligtenberg L. Love me Tinder: Untangling emerging adults' motivations for using the dating application Tinder. Telemat. Inform. 2017, 34:67-78.
30. Gustafson DH, Hawkins RP, Boberg EW, McTavish F, Owens B, Wise M, et al. CHESS: 10 years of research and development in consumer health informatics for broad populations, including the underserved. Int J Med Inform. 2002, 65(3): 169-77.
31. Caceres C, Gomez EJ, Garcia F, Gatell JM, del Pozo F. An integral care telemedicine system for HIV/AIDS patients. Int J Med Inform. 2006, 75(9): 638-42.
32. Cell-Life. The Cell-Life Solution. Available online: http://www.celllife.org/ (Accessed on 23-Jan-2023)
Received: 10 February 2023/ Accepted: 15 May 2023 / Published:15 June 2023
Citation: Diaz S, Cooper M, Molina Y, Zablah I, García Loureiro A, Agudelo-Santos C, Madrid M, Madrid M, Rodriguez J, Urmeneta J, Valle Reconco J. Information and communication technologies (ICT) access indicators in the LGBTQ+ population with a high risk of contagion by acquired immunodeficiency virus (HIV) in Honduras Revis Bionatura 2023;8 (2) 34. http://dx.doi.org/10.21931/RB/2023.08.02.34