2020.05.02.5
Files > Volume 5 > Vol 5 No 2 2020
INVESTIGATION / RESEARCH
Clinical and Epidemiological characterization of an outbreak by carbapenemase-producing Klebsiella pneumoniae. January-March, 2017, Portoviejo, Ecuador.

Eduardo Silva1, Diana Milanés2 and Martha Fors3
Available from: http://dx.doi.org/10.21931/RB/2020.05.02.5
ABSTRACT
Infection Control reported three cases of Kpn-KPC with a probable relation among them in the adult intensive care unit UCI-A in the hospital “Dr. Verdi Cevallos Balda” from Portoviejo, Manabi, Ecuador. This observational and descriptive study aims to characterize this outbreak, according time, space and person. Laboratory tests are analyzed, and the correlation between cases and positive result of the study is shown. Clinical epidemiological aspects of patients with Kpn-KPC carbapenemases producing Klepsiella pneumoniae infection were recorded (January to March 2017). The ICU-A Adult Intensive Care Unit and family environment are a probable factor of dissemination of the disease. The isolation of KPC is an alternative to clinical suspicion. The implementation of infection control measures is essential to reduce nosocomial transmission of Kpn-KPC.
Keywords: Kpn-KPC, epidemic outbreak, infected case, colonized case.
INTRODUCTION
Klebsiella pneumoniae producing carbapenemase type KPC (Kpn-KPC) is part of the emerging pathogens, with high capacity for in-hospital dissemination. The resistance of this species to third-generation cephalosporins through the production of extended-spectrum beta-lactamases (ESBL) is frequent, placing carbapenemes as the treatment of choice in infections caused by these isolates1. However, in 1996, the first clinical isolation of carbapenemase-resistant K. pneumoniae was performed, through the production of carbapenemase type KPC in North Carolina, United States. From this first isolation, outbreaks are recognized in various regions of the world, identifying a worldwide dominant clone, the ST258 2.
Ecuador begins in 1985, from the publication of a Manual of Standards and Procedures by the Ministry of Health, and three years later there is the construction of a committee in the National Directorate of Epidemiology, in 2006 the Ministry of Public Health established the Norms of Control and Prevention of nosocomial infections.
In Eugenio Espejo Specialties Hospital in the City of Quito, an observational, retrospective and descriptive study was carried out of a series of 57 cases that register cultures with KPC type carbapenemase-producing Klebsiella pneumoniae isolates. The diagnosis was made between July and December of 2014. We worked with the universe of 59 patients with isolation of Klebsiella pneumoniae producing KPC type carbapenemases according to the daily census issued by the Statistics Unit of the said hospital.
Due to the exclusion criteria used, work was done with a total of 57 patients who died from this cause; the median age corresponded to 58, highlighting the group between 19 and 65 years of age (n = 30). The hospital stay time reached (p10 = 30) and (p90 = 79.6). The proportion of patients who received surgical procedures was 0.877.
In 40 cases of the deceased, the germ isolates came from orotracheal secretions, bronchoalveolar aspirate, or pleural fluid (70.2%); of these, 37 patients presented mechanical ventilation (64.9%). In 22 of the deceased cases, the isolates were performed in the secretion of surgical wounds or secretion of bedsores (38.6%). In 11, their isolates were presented in blood cultures, and in 4, they were isolated in urinary tract cultures 3.
There is no history of this type of outbreak at the Hospital "Dr. Verdi Cevallos Balda” of Portoviejo, and neither any kind of study carried out in it. Hence, the objective of the present study is to epidemiologically characterize an IH Intrahospital outbreak by Kpn-KPC in hospitalized patients the ICU-A of the Hospital“Dr. Verdi Cevallos Balda”. For the present study, the exceptional and unexpected increase in the number of Kpn-KPC cases was considered as an outbreak since two cases of Kpn-KPC infection and one case colonized by Kpn-KPC and the final decision of the Control Committee for Infections prevailed at the time of declaring an outpatient outbreak. A propagation pattern that favors the hypothesis of transmission from person to person was considered.
MATERIAL AND METHODS
The Hospital “Dr. Verdi Cevallos Balda” is a provincial hospital located in the city of Portoviejo, province of Manabí, Ecuador, and has 140 hospitalization beds distributed in surgical, clinical, and intensive care areas.
Study period
From the detection of the index case in January 2017 to the outbreak closure in March 2017.
Study design
Observational and descriptive study. The relevant epidemiological and clinical aspects of patients with Kpn-KPC infection (cases) were recorded. All patients hospitalized in ICU-A with Kpn-KPC isolation from a clinical sample plus clinical and laboratory manifestations of the disease were defined as a case. It was described as colonization to the separation of this agent in surveillance rectal swab samples in patients without clinical or laboratory manifestations of the disease. Evolution was defined as: favorable (resolution of symptoms and signs of infection), attributable unfavorable nonattributable (death in the context of active infection plus positive culture outcome), and unfortunate (mortality in the context of active infection plus the result of negative culture).
A multidisciplinary infection prevention and control strategy were immediately implemented when the outbreak was detected and continued until the outbreak was declared over.
Statistical analysis
A descriptive statistical analysis of the variables was performed.
RESULTS
During the study period, 2 cases of infection and 1 of colonization by Kpn-KPC were documented. The clinical characteristics and the evolution of the cases are described in Table 1.
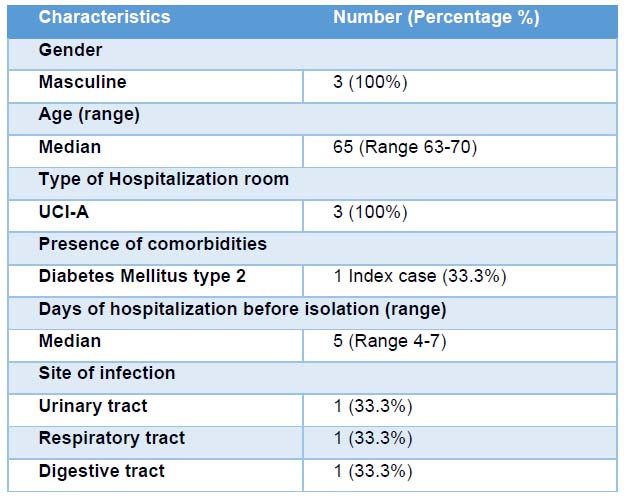
Table 1. Clinical and epidemiological characteristics of 3 cases of Kpn-KPC-producing Klebsiella pneumoniae infection.
The first case was detected on January 25, 2017, in the intensive care unit (ICU-A), in a patient admitted to the hospital with a diagnosis of septic Shock of nondetermined focus. The second case is detected in the intensive care unit (ICU-A) on January 30, 2017, in a patient admitted with a diagnosis of chest trauma. The third colonized case is detected in the intensive care unit (ICU-A) on January 30, 2017, with a diagnosis of Chronic Obstructive Pulmonary Disease COPD.
The hospitalization room for patients at the time of diagnosis of Kpn-KPC infection was the adult intensive care unit (ICU-A). The overall mortality was 66.6%, while the mortality attributable to Kpn-KPC infection was 33.3% of the cases. (Table 2)
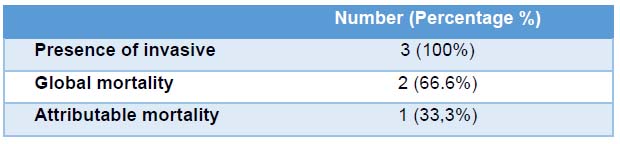
Table 2 Mortality
Within the strategies implemented for the control of the outbreak, surveillance swabs were performed in the three patients, of which 1 (33%) was colonized.
Among the strategies used to control the outbreak are the following: the education of the patient, family members, and health personnel, intensification of the control of compliance with isolation measures (handwashing, use of gloves and disposable gowns). It was possible to have staff that only worked in the UCI-A, besides the cleaning staff that was exclusive and unique for this room. It can be considered that these measures were effective in controlling the outbreak since, once implemented, there were no more cases of infection with Kpn-KPC in hospitalized patients or ICU-A staff. The outbreak closes with the death of the second infected case on 03/04/2017.
DISCUSSION
Our epidemiologic study describes the evolution of carbapenem-resistant K. pneumoniae over time in a hospital in Portoviejo, Ecuador. The hospital's Infection Control Committee declares an outbreak of Kpn-KPC with a high dissemination capacity from patient to patient in the ICU-A Intensive Care Unit due to its relationship between time, space, and person. One patient in the 3 cases of our study presented comorbidities such as type 2 diabetes mellitus and risk factors before hospitalization and administration of antimicrobials. These findings coincide with previous studies that evaluated risk factors for the acquisition of Kpn-KPC infections.
In one of them, the presence of severe disease and the previous use of antimicrobials, mainly cephalosporins and quinolones, were identified as risk factors 4.
The sensitivity of the Kpn-KPC isolates of patients during the outbreak decreased therapeutic options, the empirical treatment being inadequate in most cases. The optimal treatment for infections caused by Kpn-KPC is not established. Moreover, the clinical data are minimal and are mainly based on case reports or small case series 2. Colistin was the most frequently used antimicrobial in our patients.
Although all patients received a targeted and adequate antibiotic treatment, the overall mortality was high 2 of 3 patients for 66.6%.
The strategies used to control Kpn-KPC infections, such as increased environmental cleanliness, surveillance cultures, contact precautions, and prudent use of antimicrobials, were necessary to control the outbreak. The implementation of surveillance swabs allowed to identify patients with colonization with Kpn-KPC, which are an essential source of transmission during nosocomial outbreaks 5.
The ICU-A adult Intensive Care Unit room and the family environment are a likely factor of dissemination of the disease. The isolation of KPC is an alternative to clinical suspicion. The implementation of infection control measures is essential to reduce nosocomial transmission of Kpn-KPC.
To conclude, it is essential to note that the Infection Control team and health personnel must be alerted to identify the risk factors for Kpn-KPC infection, and thus improve the detection of probable cases and establish an adequate empirical antibiotic treatment. In this way, preventive measures could be taken earlier and so avoid the patient-to-patient spread of this menacing bacterium and prevent future outbreaks in the hospital.
CONCLUSIONS
The implementation of infection control measures is essential to reduce nosocomial transmission of Kpn-KPC. Infection Control team and health personnel must be alerted to identify the risk factors for Kpn-KPC infection, and thus improve the detection of probable cases and establish an adequate empirical antibiotic treatment. In this way, preventive measures could be taken earlier and so avoid the patient-to-patient spread of this menacing bacterium and prevent future outbreaks in the hospital. Intensive Care Unit room and the family environment are a probable factor of dissemination of the disease. The isolation of KPC is an alternative to clinical suspicion.
Limitations
Our study has some limitations. The main one is the sample size. The delusion of these infections is relatively low. Exposure to previous antibiotics was not collected. It was not possible to obtain molecular and phenotypic results of the samples of these patients.
Acknowledgments
To all hospital health staff “Dr. Verdi Cevallos Balda” from Portoviejo, Manabí, Ecuador, who participated in the care, diagnosis, supervision, and monitoring of actions performed on patients during the outbreak by Kpn-KPC.
Conflict of Interest
The author declares no conflict of interest.
REFERENCES
1. Asensio A, Oliver A, González-Diego P, Baquero F, Pérez-Díaz JC, Ros P, et al. Outbreak of a multiresistant Klebsiella pneumoniae Strain in an Intensive Care Unit: antibiotic use as risk factor for colonization and Infection. Clin Infect Dis. 2000;30:55–60.
2. Hirsch E, Tam V. Detection and treatment options for Klebsiella pneumoniae carbapenemases (KPCs): an emerging cause of multidrug-resistant infection.J Antimicrob Chemother. 2010;65:1119–25.
3. Buitrón G., Quezada I., Coronel A., Rosero C.,Armijos L., Dávila E., Comportamiento de casos de Klebsiella Pneumoniae productora de Carbapenemesas en pacientes de un Hospital de tercer nivel de la ciudad de Quito. Rev Med Reflexiones 2015; 16: 9-13.
4. Gasink LB, Edelstein PH, Lautenbach E, Synnestvedt M, Fishman NO. Risk factors and clinical impact of Klebsiella pneumoniae carbapenemase-producing K. pneumonia. Infect Control Hosp Epidemiol. 2009;30:1180–5.
5. Lledo W, Hernández M, López E, Molinari OL, Soto RQ, Hernández E, et al., Centers for Disease Control and Prevention (CDC). Guidance for control of infections with carbapenem-resistant or carbapenemase-producing enterobacteriaceae in acute care facilities. MMWR Morb Mortal Wkly Rep. 2009;58: 256–60.
Received: 23 March 2020
Accepted: 10 April 2020
Eduardo Silva1, Diana Milanés2 and Martha Fors3
1. Eduardo Silva. Epidemiologyst. Dirección Nacional de Salud de la Policía Nacional, Quito, Ecuador. [email protected]. ORCID 0002-7956-9819
2. Diana Milanés. Medical doctor. Instituto Nacional de Salud Pública Leopoldo Izquieta Pérez, Quito, Ecuador. [email protected]. ORCID 0003-0139-1720
3. Martha Fors. Phd. Universidad de Las Américas, Quito, Ecuador. ORCID 0000-0002-0844-199X
Corresponding author
Martha Fors. Universidad de Las Américas. Quito, Ecuador
Avenida de Los Granados, Vía a Nayón. Quito, Pichincha, Ecuador. Código postal 17022
Email [email protected]