2023.08.02.81
Files > Volume 8 > Vol 8 No 2 2023
Evaluation of mutans streptococci concerning oral health in the saliva of pregnant women

Al-zahraa J. Jassim 1*, Zainab A. Aldhaher 2
1 Department of Basic Science, College of Dentistry, University of Baghdad, Iraq
2 Department of Basic Science, College of Dentistry, University of Baghdad, Iraq
* Correspondence: [email protected].
Available from: http://dx.doi.org/10.21931/RB/2023.08.02.81
ABSTRACT
Pregnancy is a physiological condition that affects a woman's life, including susceptibility to oral disease. Increased levels of female hormones impact the growth of periodontal pathogenic bacteria. In several mutants, Streptococci levels are said to be greater during Pregnancy. Thus, the cariogenic bacteria predominating in plaque and saliva will develop more acids through fermentation, leading to dental caries. The present study aimed to assess (Decay and Decayed, Missing and Filled Surface) value and mutans streptococci counts in pregnant and non-pregnant women. The method was applied to 80 women, with an age range of 20 to 30 years. The study group comprised 60 pregnant women divided into three equal trimester groups (20 pregnant women in each trimester), while the control group consisted of 20 married non-pregnant. The salivary samples were collected under standardized conditions for microbiological analysis and oral examination done by caries experience (Decay and Decayed, Missing and Filled Surfaces). Results revealed that Decayed, Missing and Filled Surfaces value and mutans Streptococci count was higher in (study groups) in comparison to (control group) in addition to the correlation between the viable count of mutans streptococci (CFU×105 /ml) and DMF appeared positive significant result in this study.
Keywords: Pregnant women, DMFs, mutans streptococci.
INTRODUCTION
Pregnancy is a temporary physiological condition in which a woman's body undergoes many hormonal changes. These effects are generalized, and there are several oral alterations: 1.
Nearly all bodily systems undergo functional and biochemical changes during Pregnancy. The hormonal changes related to Pregnancy make women more vulnerable to oral problems such as dental caries, cariogenic flora and periodontal disease. During Pregnancy, it is discovered that the mutans count is particularly elevated 2. It is believed that changes in saliva composition, gastric reflux and inadequate oral healthcare during Pregnancy may raise the risk of caries development 3.
Saliva plays a crucial role in the formation of teeth caries; it shields the enamel from the decline of phosphate and calcium ions from the tooth surface by forming a tooth pellicle. The pellicle in saliva serves as a hindrance of protection to assist in the prevention of demineralization, remineralization promotion, the maintenance of the oral cavity's pH balance and washing away food residue from the tooth surfaces 4.
During Pregnancy, rises in levels of female hormones cause the development of periodontal pathogenic bacteria 5, 6. However, it is believed that during Pregnancy, the proportion of mutans Streptococci is increased 7. Some researchers reported that mutans Streptococci significantly increased in pregnant women, a recognized cause of dental caries 8, 9. If plaque and saliva include cariogenic bacteria, it will increase the acids they produce through carbohydrate fermentation. Then, it will increase the bacterial colony and form a biofilm on the tooth surface 10.
MATERIALS AND METHODS
The current study was conducted from December 2021 to March 2022. Collecting samples was conducted from the Medical City / Baghdad Hospital / Women's Consultant and Al-mustansiriyah Health Center in Baghdad. Eighty women aged 20 – 30 were enrolled in this study; 60 pregnant women represented study groups and were divided into three groups: 20 from the first trimester, 20 from the second trimester, 20 from the third trimester, and 20 married non-pregnant women represented (control group). Oral examination was done by application of Decayed, Missing and Filled index according to the criteria of who 11.
Microbiological part
In the morning (9-11 a.m.), saliva was collected for each woman. Under a standardized situation, salivary samples were collected according to the instructions constructed by Navazesh 12, and samples were taken from the study group and the control group.
Saliva samples were homogenized for 1 minute in a vortex mixer. Ten-fold serial dilutions were created by adding 0.1 ml of homogenized saliva to 0.9 ml of sterile phosphate buffer saline (pH=7), then 0.1 ml of saliva was taken from the dilution (10-1 – 10-5) and disseminated in duplicate using sterile microbiological spreader on MSB agar. In an anaerobic jar with a gas pack, the plates were incubated anaerobically for 48 hours at 37°C, then aerobically for 24 hours at 37°C 13.
Identification was carried out using Gram stain result, catalase test, colony morphology, and biochemical test. A bacterial colony count and a carbohydrate fermentation test for MS were also performed.
RESULTS
Carie's experience in study groups and control group
Table 1: demonstrated Decay (D) and Decay missing fillings (DMFs) of study and control groups. The result of Decay (D) revealed that there were positive significant differences among the four groups and the mean value of first-trimester group was (3 ± 1.97), (7.25 ± 2.31) for the second-trimester group, (11.15± 3.09) for third-trimester group and (3.1 ± 1.86)for control group respectively while the result of DMFs revealed that there was positive significant differences among the four groups and the mean value of first-trimester group was (8.90 ±2.59), (13.85±3.45) for the second-trimester group, (24.55± 4.12) for third-trimester group and(9.50 ± 4.63)for Healthy control.
Comparison between intergroup for the Decay
Table 2 revealed the comparison between intergroups of Decay by using the Tukeys test. The results showed that there were significant differences. The mean difference between the first trimester and second trimester was 4.25 (0 .0000**), 8.15 (0.0000**) between the first and third trimester, 3.90 (0.0000**)between second and third trimester, 4.15 (0.0000**) between second trimester and control, 8.05 (0.0000**)third trimester and control. At the same time, there was no significant difference, and the mean difference between first trimester and control was 0.10 (0.999).
Comparison between intergroup for the DMFs
Table 3 compared the intergroup of Decay missing fillings using the Tukeys test. The results showed that there were significant differences and the mean difference between first trimester and second trimester was 4.95 (0.0005**), 15.65 (0.0000**) between first and third trimester, 10.70 (0.0000** ) between second and third trimester, 4.35 (0.0027**) between second trimester and control, 15.05 (0.0000**) between third trimester and control. At the same time, there was no significant difference between first trimester and control, and the mean difference was 0.60 (0.958).
The viable bacterial count of mutans Streptococci (CFU/ml) in study groups and control group
Table 4 and Figure 1: The viable MS count among the studied and control groups. This research using the ANOVA test revealed significant differences among groups in the viable count of MS (CFU/ml×105). The mean value of the first-trimester group was 53.35 (12.01), 70.45 (8.26) for the second-trimester group, 91.65 (7.70) for third-trimester group and 50.15 (16.68 )for the control group respectively.
Comparison of Mutans Streptococci count (CFU) between all pairs of groups
Table 5 compares the intergroup of the viable bacterial count of MS (CFU/ml×105 ) using the Tukey test. The results showed that there were significant differences. The mean difference between the first and second trimesters was 17.10(0.0000**), 38.30 (0.0000**) between the first and third trimesters, 21.20(0.0000**) between the second and third trimesters, 20.30(0.0000**)between second trimester and control, 20.30(0.0000**) between third trimester and control. At the same time, there was no significant difference between first trimester and control, and the mean difference was 3.20(0. 823).
Correlation between bacterial count and caries experiences
Table 6 shows the correlation among viable bacterial count and DMFs for study groups. The results revealed that there was a positive significant correlation and the r-value was 0.982(0.000**) between viable bacterial count (CFU) and DMFs for trimester 1, 0.909(0.000**) for trimester 2 and 0 930 (0.000**) for trimester 3.
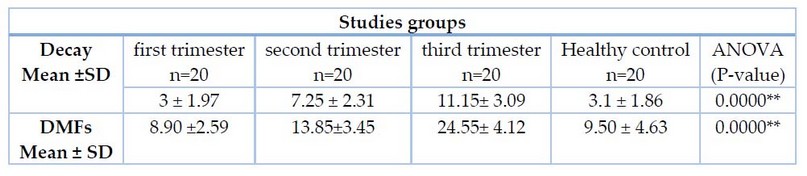
Table 1. Carie's experiences in study and control groups
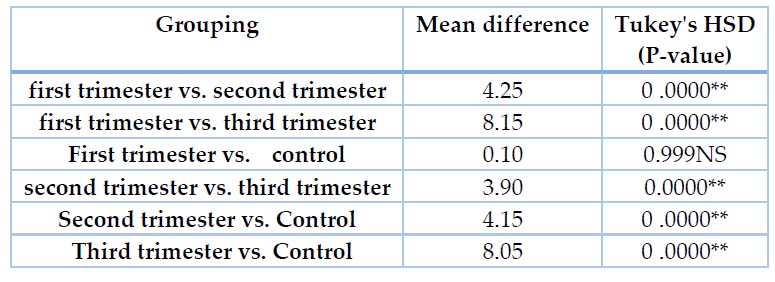
Table 2. Intergroup comparisons of mean Decay between all pairs of groups.
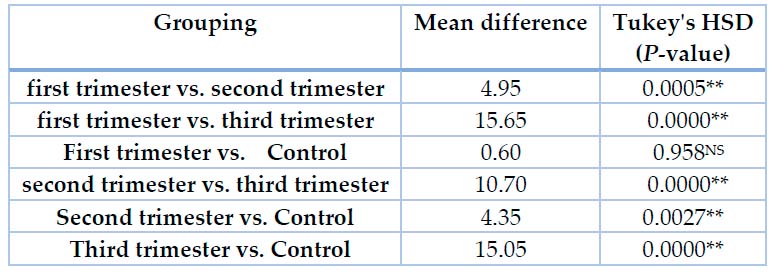
Table 3. Intergroup comparisons of mean DMFs between all pairs of groups.
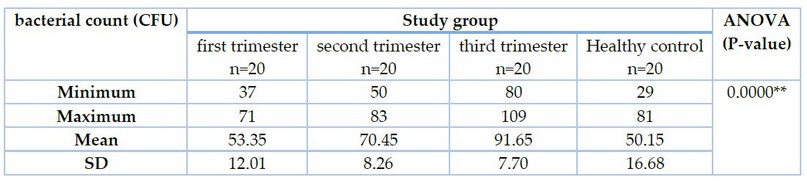
Table 4. Mean differences in viable bacterial count in study and control groups.
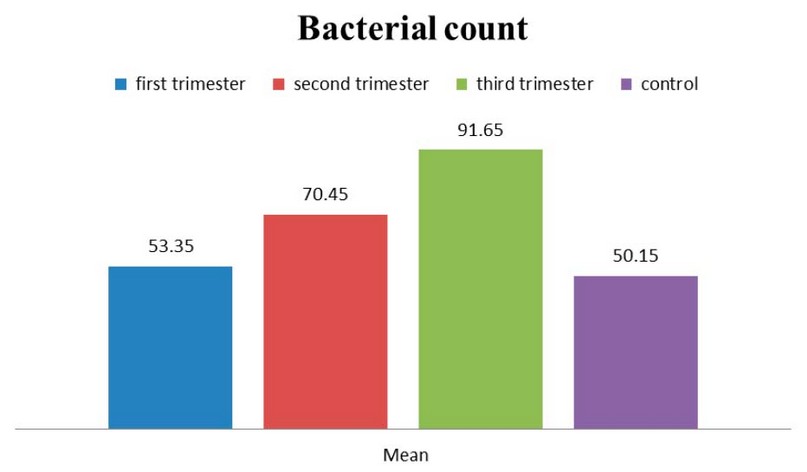
Figure 1. Mean differences in viable bacterial count (CFU) between study and control groups.
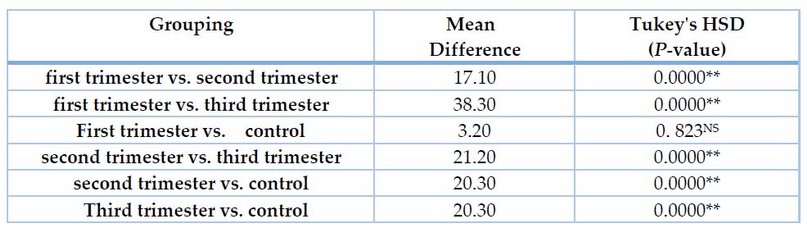
Table 5. Inter group's comparisons of mean bacterial count (CFU) between all pairs of groups.

Table 6. Shows the correlation between bacterial count (CFU) and DMFs for a study group.
DISCUSSION
Caries experience (D, DMFs)
Pregnancy produces a series of changes in the oral cavity 14, the most prevalent of which are modifications in saliva's quality and quantity, erosions, dental caries, pyogenic granulomas, and gingival hyperplasia 15.
This study used the DMF index because it measures caries surfaces rather than teeth and is more sensitive 16. The findings obtained from this study revealed that the Caries experience (D, DMFs) value was higher in pregnant women groups than in the married non-pregnant women group (control group). These results agreed with previous studies that found that dental caries experience (D, DMFS) was higher among pregnant women17, 18 On the other hand, contrary to others who found that DS fraction value decreased as the pregnancy progressed19. The results of the current study also showed that the highest value of Caries experience (D, DMFs) was seen in the third-trimester group, followed by the second-trimester group. In contrast, the caries experience (D, DMFS) of the first trimester was slightly higher with a non-significant difference when compared to the control group; these results may be explained by the fact that during Pregnancy, the mouth is exposed to stomach acid, which might damage tooth enamel.
Additionally, acid reflux and vomiting can be caused by morning sickness during Pregnancy and pressure on the gravid uterus so that pregnant women can develop dental caries and enamel erosions 20. These results are further supported by the fact that pregnant women may be interested in foods like carbohydrates and sweets, neglected tooth brushing, and their dental or oral health in general 21. Also, salivary flow rate and pH decrease during Pregnancy can lead to caries formation 22.
The Caries experience (D, DMFs) of the current study increased during the pregnancy progression; this may be due to hormone changes, anxiety and stress. Karnik explored the pregnant estrogen and progesterone rates (estriol, estradiol and estrone) rise gradually to a large extent because these hormones were produced by placental. Pregnancy also increases beta-endorphin, cortisol, and human chorionic gonadotropin (HCG), especially during the third trimester. During Pregnancy, the estradiol and estriol (biologically active forms of estrogen) rise by 100 and 1000 times, respectively. As a result, women experience physiological variations that result in adaptive modifications on both the systemic and oral domains 23, 24. The salivary flow rate decreases during the second trimester due to higher HCG levels. During Pregnancy, the salivary flow rate was reduced due to a significant rise in progesterone and human chorionic somatomammotropin (HCS) levels 25, 26. Also, Elevated progesterone lowers the plasma bicarbonate rate, reducing saliva's pH 27. Pregnant women's salivary pH and buffering capacity reach their lowest points during the third trimester, during which elevated levels of Mutans streptococci increase the chance of caries incidence 28. These reasons explain that (D, DMFs) had the highest value in the third trimester, followed by the second and first trimesters, respectively.
The viable count of mutans streptococci bacteria (CFU/ml) in the saliva of pregnant women and married non-pregnant women
The hormonal alteration during Pregnancy raises a woman's vulnerability to oral infection; at the same time, a decline of pH in saliva leads to an increase in cariogenic flora, especially mutans streptococci 29,30,31.
The results of the current study showed that the mean of salivary mutans streptococci count was higher in pregnant women groups compared to the non-pregnant group (control group), and the highest mean value of MS count was seen in the third-trimester group, followed by the second-trimester group. In contrast, the mean value of MS count in the first-trimester and non-pregnant women (control group) was approximately the same.
The current study's findings followed the results of other researchers 9, 32, 33 who discovered that the MS colony count in pregnant women's saliva was higher than in non-pregnant women's. The mean mutans Streptococci colony count in pregnant women statistically differed between trimesters. He found that the third trimester of Pregnancy had a greater mean than the first and second trimesters, but the difference between the first and control was not statistically significant.
The correlation between DMFS and mutans streptococci count (CFU/ml)
There is a significant positive relationship between the viable count of mutans streptococci (CFU×105 /ml) and DMFs in this study for all the study groups (first-trimester group, second-trimester group, third-trimester group).
Results of the Mutlak study informed that dental caries experience (D, DMFS) was higher among pregnant women 18. From all mentioned, dental caries appeared more severe among pregnant women than non-pregnant women; this is probably because of stress and psychological state 35,36.
CONCLUSIONS
Mutans streptococci count on the saliva of pregnant and non-pregnant women can be used as a diagnostic marker for predicting dental caries. These results were in agreement with previous studies that reported that the number of certain salivary cariogenic microorganisms, such as mutans streptococci, might increase through Pregnancy; at the same time, there is a drop in a buffer effect, and salivary PH was reported that might predispose to teeth decay. However, no study recorded a statistically significant correlation between MS count and DMFs.
REFERENCES
1. Marla, V.; Srii, R.; Roy, D.K. Ajmera H.The Importance of Oral Health during Pregnancy: A. Medical Express.2018; DOI: 10.5935.
2. Chickanna, R.; Prabhuji, M.; Nagarjuna, M. Host-bacterial interplay in periodontal disease. Journal of the International Clinical Dental Research Organization. 2015;7(1): 44-50.
3. Villa, A.; Abati, S.; Pileri, P.; Calabrese, S.; Capobianco, G.; Strohmenger, L.; Ottolenghi, L.; Cetin, I.; Campus, GG Oral health and oral diseases in Pregnancy: A multicentre survey of Italian postpartum women. Australian Dental Journal. 2013;58(2), 224-9.
4. Hemadi, A.S.; Huang, R.; Zhou, Y.; Zou, J. Salivary proteins and microbiota as biomarkers for early childhood caries risk assessment. International Journal of Oral Science. 2017;9 (11): e1.
5. Watanabe, T.; Nukazuka, A.; Hiramoto, I. Survey regarding oral care in pregnant women in Hospital A. Akita Journal of Maternal Health. 2007; 21:13-17.
6. Watanabe, T.; Nukazuka, A.; Kurauchi, J. Investigation into oral health condition and influence of Prevotella intermedia during Pregnancy. Bulletin of School of Health Sciences, Akita University. 2006; 14(2): 17-28.
7. Ishihara-Shinga, C.; Nakai, Y.; Ying, JI. Salivary Mutans Streptococci Levels, History of Smoking and Diet among Japanese Pregnant Women. Pediatric Dental Journal. 2007;45(5):584-592.
8. Molnar-Varlam,C.; Cristina, M.V.; Loana-Gabriela, B.; Tohati, A. Risk assessment of caries in Pregnancy. Acta Medica Marisiensis 2011;57, 685–689.
9. Kamate, W.I.; Vibhute, N.A.; Baad, RK Estimation of DMFT, Salivary Streptococcus Mutans Count, Flow Rate, Ph, and Salivary Total Calcium Content in Pregnant and Non-Pregnant Women: A Prospective Study. J Clin Diagn Res. 2017 11(4): 147-151.
10. Guo, L.; Shi, W. Salivary biomarker of caries risk assessment. J Calif Dent Assoc. 2013; 41(2): 107–118.
11. WHO. Oral health surveys basic methods. 3rded. World Health Organization. Geneva, Switzerland, 1987.
12. Navazesh, M.; Kumar, S.K. Measuring salivary flow: challenges and opportunities. J Am Dent Assoc.2008;139:35-40.
13. Holbrook, W.; Beighton, D. Streptococcus mutans levels in saliva and distribution of serotypes among 9-year-old Icelandic children. Scand J Dent Res. 1986;95(1):37-42.
14. Cheek, TG; Gutsche, BB Maternal physiologic alterations during Pregnancy. In: Shnider SM, Levinson G. eds. Anesthesia for obstetrics. Williams and Wilkins, Baltimore.1993,3–19.
15. Patil, S.; Thakur, R.; Madhu, K.; Paul, S.T.; Gadicherla, P.Oral health coalition: knowledge, attitude, practice behaviors among gynecologists and dental practitioners. Journal of International Oral Health.2013; 5(1): 8–15.
16. Manji, F.; Fejerskove, O.; Baleum,V. The pattern of dental caries in an adult rural population. Caries Res.1989;23(1):55-62.
17. Al-Azzawi, L.; Yas, B.A.Evaluation of dental caries experience and treatment needs of pregnant women in Baghdad governorate . J Bagh Coll Dentistry. 2007;19(1): 107-111.
18. Mutlak, Q.N.; Yas, B. A. Dental caries severity in relation to selected salivary variables among a group of pregnant women in Baghdad city/Iraq.J Bagh College Dentistry. 2016; 29(2)
19. Papp, E.; Kengyeli, I.; Banoczy, J.; Csordas, T. Longitudinal study of the dental status of pregnant women under prenatal care. Fogorv Sz. 1990;83(7):199-204.
20. Silk, H.; Douglass, A.B.; Douglass, J.M.; Silk, L. Oral health during Pregnancy. American Family Physician.2008;15,77(8):1139-44.
21. Rakchanok, N.; Amporn, D.; Yoshida, Y.; Harun-Or-Rashid, M.; Sakamoto, J. Dental caries and gingivitis among pregnant and non-pregnant women in Chiang Mai, Thailand. Nagoya J Med Sci. 2010;72(1-2):43-50.
22. Tulunoglu, O.; Demirtas, S.; Tulunoglu, I. Total anti-oxidant levels of saliva in children related to caries, age, and gender. Int J Paediatr Dent.2006; 16(3), p186-91.
23. Karnik, A.A.; Pagare, S.S.; Krishnamurthy, V.; Vahanwala, S.P.; Waghmare, M. Determination of salivary flow rate, pH, and dental caries during Pregnancy: A study. J Indian Acad Oral Med Radiol.2015;27(3): 372-376.
24. Hendrick, V.; Altshuler, L.L.; Suri, R. Hormonal changes in the postpartum and implications for postpartum depression. Psychosomatics.1998;39:93-101.
25. Kaliliou, M.V. Saliva ovulation pregnancy tester. Br J Gynecol.2002;11:20-3.
26. Al-Nuaimy, K.M.; Al-Doski, F.S. Pregnancy-related changes in oral health and human unstimulated whole saliva. Al-Rafidain Dent J.2003;3:108-15.
27. Grossman, L.I.; Brickman, B.M. Some observations on the pH of saliva. J Dent Res.1987;16:409-16.
28. Laine, M.; Tenovuo, J.; Lehtonen, O.P.; Ojanotko- Harri, A.; Vilija, P.; Tuohimma, P. Pregnancy-related changes in human whole saliva. Arch Oral Biol.1988;32:913-7.
29. Soderling, E.; Isokangas, P.; Pienihakkinen, K.; Tenovuo, J. Influence of maternal xylitol consumption on acquisition of mutans streptococci by infants. J. Dent. Res . 2000;79(3): 882-7.
30. HerreraG, C.L.; PantojaF, P.; LaMaza, T.; Sanhueza, C.A.; SalazarN, L.A. Microbiologic and molecular diagnostic of cariogenic bacteria in pregnant women from the Araucania Region of Chile. Rev Chilena Infectol. 2008; 24(4):270-5.
31. Oztruk, L.K.; Akyuz, S.; Garan, A.; Yarat, A. Salivary and dental - oral hygiene parameters in 3rd trimester of Pregnancy and early lactation: the effect of education.Marmara Dental Journal. 2013;1:01-08.
32. Purushothama, P.; Ravi, S.; Ajjapanahalli, K.A. Estimation of Streptococcus Mutans Count in Saliva of Pregnant Women- A Case-Control Study· Indian Journal of Public Health Research and Development .2014;5(4):263.
33. Wagle, M.;Basnet, P.; Vårtun, Å.; Acharya, G. Nitric Oxide, Oxidative Stress and Streptococcus mutans and Lactobacillus Bacterial Loads in Saliva during the Different Stages of Pregnancy: A Longitudinal Study. Int J Environ Res Public Health. 2021; 18(17): 9330.
34. Vadikas, G.; Lianos, C .Correlation between Pregnancy and dental caries. Hell Stomatol Chron.1988;32(4):267-72.
35. Taani, D.Q.; Habashneh, R.; Hammad, M.M.; Batieha, A.The periodontal status of pregnant women and its relationship with socio-demographic and clinical variables. Journal of Oral Rehabilitation. 2003; 30: 440–445.
36. Chłapowska, J.; Opydo-Szymaczek, J. Dietary and hygienic aspects of fluoride exposure in pregnant women.Ann Acad Med Stetin. 2004; 50(1): 19–22.
Received: May 15, 2023/ Accepted: June 10, 2023 / Published: June 15, 2023
Citation: Al-zahraa J J, Aldhaher Z A. Evaluation of mutans streptococci concerning oral health in the saliva of pregnant women.Revis Bionatura 2023;8 (2) 81. http://dx.doi.org/10.21931/RB/2023.08.02.81