2021.06.04.23
Files > Volume 6 > Vol 6 No 4 2021
INVESTIGATION / RESEARCH
Prevalence of antibodies in Iraqi Urinary Tract Infection patients using radial immunodiffusion (RID) assay

Saja Mohammed Mohsen1* Anas Wisam malik 1
Available from: http://dx.doi.org/10.21931/RB/2021.06.04.23
ABSTRACT
Urinary Tract Infection (UTI) is an infection every place in the urinary tract that may be in the urethra, bladder, or kidneys by microbes. Greatest UTIs are affected by bacteria, but some are affected by fungi and, in rare cases, by viruses. UTI is the most significant common infection in humans. This study deals with the prevalence of antibodies in UTI patients; this study aims to determine the level of antibodies in UTI patients and compare with healthy controls by using the radial immunodiffusion (RID) test. The study was done during the period November 2019 to April 2020 on UTI Iraqi patients. The study included 40 patients and 20 healthy controls. Results show UTI infection occurs in females more than males also; the mean age is 40 years. All the patients with UTI showed decreased IgM serum levels and increased IgG compared with the control group. IgG, IgG, and IgM showed high significance between two UTI patients and the control group groups, while IgM doesn’t show significant differences between study groups.
Keywords: Urinary Tract Infection, RID, antibodies
INTRODUCTION
Urinary tract infections (UTIs) are common bacterial infections, with nearly more than one hundred and fifty million individuals infected yearly1. In the United States, estimated 10.5 million clinic cases with UTI symptoms and 2–3 million cases visit the emergency department 2–4.
The urinary tract includes kidneys, ureters, bladder, and urethra. Several natural factors are secret with urine from the urinary tract for protecting against all infection agents; also, the anatomical and mechanical barriers have a significant role, such as the glycoprotein plaque uroplakins 5 and a layer of hydrated mucus 6. Furthermore, the urinary tract lining is made by immune cells and epithelial cells, which have an important role in protecting against bacterial infection and preventing bacteria from getting into the urinary tract6. UTIs are most common in females more than males, and the incidence rate has increased during the last (30) years 6.
UTIs increase in the elderly due to the immune-compromised individuals, and the urinary catheter has an essential role in increasing the percentage of infection 7.
Immunity has two types innate immunity and adaptive immunity 8-10. The individual with innate immunity has resistance against the infection. Innate immunity includes many chemical and cellular components. The infection gets in and spreads, but the person with high immunity has resistance against the bacteria 11. Adaptive immunity has two types of humoral immunity, and cellular immunity includes all the naturally acquired immunity due to infection vaccination 12-15.
Features likely to contribute to disease of the human immune system involve the responses to antigens (B- and T-cell features, PMNs), the efficiency of bacterial destruction (e.g., lysozyme, complement), and types of antimicrobial substances produced (e.g., immunoglobulins, Cytokines) 16. Immunoglobulins are a group of serum proteins with a crucial antimicrobial activity; IgM represents an indicator of recent infection, IgG levels increased in chronic infections 17.
MATERIAL AND METHODS
This study was conducted around UTI Iraqi patients during the period from November 2019 to April 2020. This study included 40 patients and 20 healthy controls.
Samples collection
Serum samples were collected from the patient in Al-Khalis General Hospital and National Laboratories in Al-Khalis District / Diyala Governorate (Iraq) from November 2019 to April 2020. After examining their urine samples by the microscope, they were divided into two groups first is patients with UTI, and the other group is healthy who does not suffer from UTI; this group is considered the control for comparison with the first group.
Estimation of antibodies
Using radial immunodiffusion test to detect levels of antibodies in serum is done by using (LTA, Italia). Normal values of antibodies were IgG (800-1800 mg/dl) and IgM (60-280 mg/dl).
Statistical Analysis
The Statistical Analysis System (SPSS) program was used to detect the effect of different factors in study parameters least significant difference, using T-test for comparing between the means value and the using of the Chi-Square test for comparing between the percentage.
RESULTS AND DISCUSSION
The patient group involved 40 patients, 8 males 20% and 32 females 80%, with a mean age of 40.60 ± 2.295 years. The healthy control group consisted of 20 subjects, 11 males ( 55%) and 9 females (45%), with a mean age of 36.80 ± 3.441 years, as seen in tables 1 and 2 explain the distribution of the two study groups according to gender and age.
Results in Tables 1 and 2 show UTI infections occur in females more than males; the mean age is 40.60 ± 2.295 years. The higher incidence of UTI in females than males might be due to a variety of factors, such as the proximity of the female urethral meatus to the anus 18. Also, most school girls are avoiding urinable in school, which is accompanied by urinary infection 19. Alternatively, vaginal flora has a vital role vaginal infection with coliforms which leads to urinary tract infection20. The female anatomic feature also contributes to higher prevalence among the female subject. This finding is agreed with earlier studies 21-22.
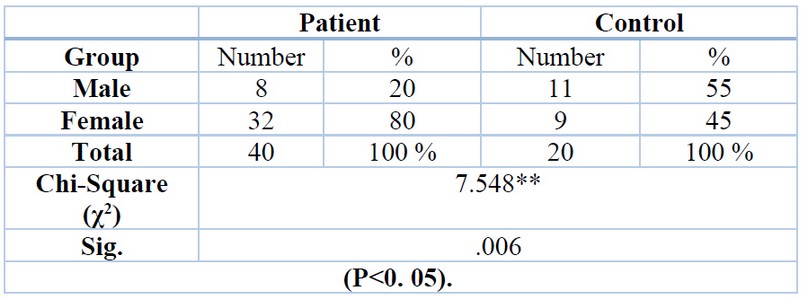
Table 1. Distribution of the two-studied group according to gender
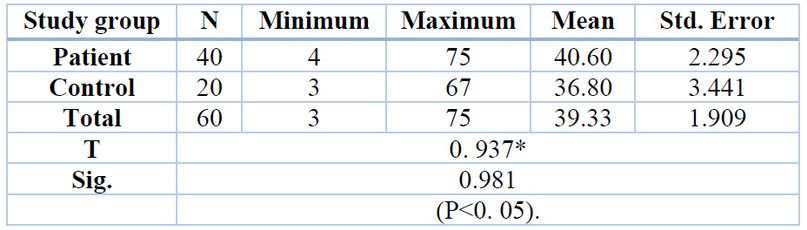
Table 2. Distribution of the two-studied group according to age
There was a significant increase in the mean concentration of IgG in sera of patients (854.82±138.79) mg/dl compared with the mean concentration of IgG in sera of the control group (616.4 ± 67.65) mg/dl. These results show high significance between two groups UTI patients and control group according to IgG while non-significant to IgM show table 3. This finding is agreed with AlSaadawi and Alkhaled (2015) 23. Elevation in serum concentration of IgG in patients suffering from UTI may be the reason for the significant increases in the concentration of complement components in patients suffering from UTI24. Higher values IgG undergo increases to protect and combat infection 24.
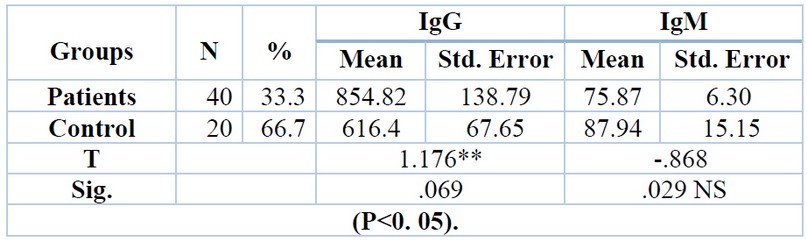
Table 3. Prevalence of IgG and IgM among UTI patients and control group
Table 4 shows the non-significant difference in gender distribution between two groups according to IgG and IgM. IgG and IgM prevalence in UTI patients was (838.82 ± 121.49) mg/dl and (70.23± 8.48) mg/dl for male IgG and IgM respectively, while in females was (858.82 ± 171.63) mg/dl and (77.28 ± 7.62) mg/dl for IgG and IgM respectively, this similar with El Mashad et al. 2017 25.
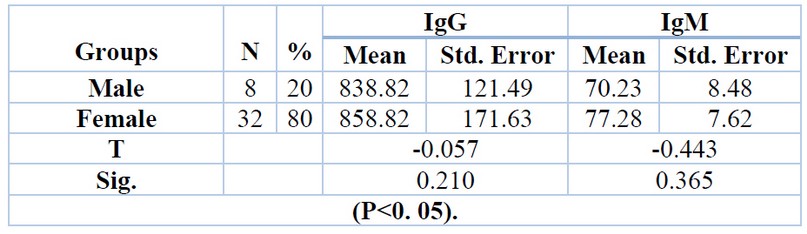
Table 4. Effect of gender on IgG and IgM prevalence in UTI patients
Non-significant between two groups (with RBC and without RBC) according to IgG and IgM. With RBC group was (823.85 ± 152.75) mg/dl and (82.01± 15.78) mg/dl for IgG and IgM respectively, while in without RBC group was (871.49 ± 199.17) mg/dl and (72.57 ± 4.93) mg/dl for IgG and IgM respectively show table 5.
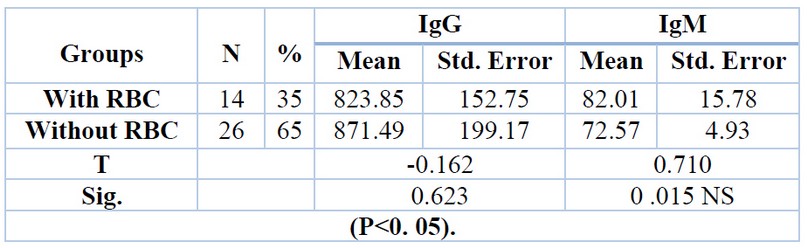
Table 5. Effect of present RBC on IgG and IgM prevalence in UTI patients
CONCLUSION
We conclude that UTI infection occurs in females more than males; the mean age is 40 years. In all patients with UTI compared to control, the IgG serum level increases and IgM serum level decreases. Serum IgG and IgM showed high significance between two groups of UTI patients and the control group according to IgG while IgM showed non-significant and serum IgG and IgM showed no significant difference in UTI patients and RBC groups.
REFERENCES
1. Stamm WE, Norrby SR. Urinary tract infections: disease panorama and challenges. The Journal of infectious diseases. 2001 Mar 1;183(Supplement_1):S1-4.
2. Schappert SM, Rechtsteiner EA. Ambulatory medical care utilization estimates for 2007. Vital and Health Statistics. Series 13, Data from the National Health Survey. 2011 1 April (169):1-38.
3. Foxman B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infectious Disease Clinics. 2014 Mar 1;28(1):1-3.
4. Foxman B. The epidemiology of urinary tract infection. Nature Reviews Urology. 2010 Dec;7(12):653-60.
5. Wu XR, Kong XP, Pellicer A, Kreibich G, Sun TT. Uroplakins in urothelial biology, function, and disease. Kidney international. 2009 1 June;75(11):1153-65.
6. Grist M, Chakraborty J. Identification of a mucin layerin the urinary bladder. Urology. 1994 1 July;44(1):26-33.
7. Nicolle LE. Urinary tract pathogens in complicated infection and elderly individuals. The Journal of infectious diseases. 2001 1 March;183(Supplement_1): S5-8.
8. Becknell B, Schwaderer A, Hains DS, Spencer JD. Amplifying renal immunity: the role of antimicrobial peptides in pyelonephritis. Nature Reviews Nephrology. 2015 Nov;11(11):642-55.
9. Hains DS, Schwaderer AL. Genetic variations in vesicoureteral reflux sequelae. Pathogens. 2016 Mar;5(1):14.
10. Kucheria R, Dasgupta P, Sacks S, Khan M, Sheerin N. Urinary tract infections: new insights into a common problem. Postgraduate medical journal. 2005 Feb;81(952):83.
11. Schilling JD, Mulvey MA, Hultgren SJ. Dynamic interactions between host and pathogen during acute urinary tract infections. Urology. 2001 1 June;57(6):56-61.
12. Cheng CH, Lee YS, Chang CJ, Lin JC, Lin TY. Genetic polymorphisms in inflammasome-dependent innate immunity among pediatric patients with severe renal parenchymal infections. PloS one. 2015 Oct 7;10(10):e0140128.
13. Lüthje P, Brauner A. Novel strategies in the prevention and treatment of urinary tract infections. Pathogens. 2016 Mar;5(1):13.
14. Mak RH, Kuo HJ. Pathogenesis of urinary tract infection: an update. Current opinion in pediatrics. 2006 Apr 1;18(2):148-52.
15. Ulett GC, Totsika M, Schaale K, Carey AJ, Sweet MJ, Schembri MA. Uropathogenic Escherichia coli virulence and innate immune responses during urinary tract infection. Current opinion in microbiology. 2013 Feb 1;16(1):100-7.
16. Akhavan Sepahi M, Hosseini R, Akhavan Sepahi A. The innate immune response during acute urinary tract infections; an overview. Caspian Journal of Pediatrics. 2018 Mar 10;4(1):282-9.
17. Al-khafaf DM. Study of some microbial and Immunological parameter in patients with Urinary Tract Infection in Al-Diwanyia city. Al-Qadisiyah Medical Journal. 2012;8(13):28-38.
18. Goldman M, Lahat E, Strauss S, Reisler G, Livne A, Gordin L, Aladjem M. Imaging after urinary tract infection in male neonates. Pediatrics. 2000 1 June;105(6):1232-5.
19. Schneede P, Hofstetter AG, Naber KG, Vahlensieck W, Ludwig M, Bach D, Bauer HW, Beyaert G, Blenk H, Bootz T, Friesen A. European Association of Urology guidelines on urinary and male genital tract infections. Der Urologe. Ausg. A. 2003 Jan 1;42(1):104-12.
20. Newman TB, Bernzweig JA, Takayama JI, Finch SA, Wasserman RC, Pantell RH. Urine testing and urinary tract infections in febrile infants seen in office settings: the Pediatric Research in Office Settings’ Febrile Infant Study. Archives of pediatrics & adolescent medicine. 2002 1 January;156(1):44-54.
21. Oluwafemi TT, Akinbodewa AA, Ogunleye A, Adejumo OA. Urinary tract infections and antibiotic sensitivity pattern of uropathogens in a tertiary hospital in South West, Nigeria. Sahel Medical Journal. 2018 1 January;21(1):18.
22 . AlSaadawi MA. Prevalence of toxoplasmosis in renal infections patients in Al-Muthanna province/Iraq. Al-Qadisiyah Journal of Veterinary Medicine Sciences. 2015 30 June;14(1):58-60.
23. NAJDAT B MAHDI SK. Relationship among Some Immunoglobulins, Complement Protein C3 and Urinary Tract Infection of Women Caused by Gram Negative Bacilli in Kirkuk, Iraq. International Journal of Current Research and Academic Review. 2016;4:99-106.
24. Weichhart T, Haidinger M, Hörl WH, Säemann MD. Current concepts of molecular defence mechanisms operative during urinary tract infection. European journal of clinical investigation. 2008 Oct;38:29-38.
25. El Mashad GM, Ibrahim SA, Abdelnaby SA. Immunoglobulin G and M levels in childhood nephrotic syndrome: two centers Egyptian study. Electronic physician. 2017 Feb;9(2):3728.
Received: 26 August 2021
Accepted: 9 October 2021
Saja Mohammed Mohsen1* Anas Wisam malik 1
1 Middle Technical University, Baquba Technical Institute, Baquba, Iraq
Corresponding author*e-mail : [email protected]