2023.08.02.50
Files > Volume 8 > Vol 8 No 2 2023
Evaluation study of the size and function of mechanical heart valve replacement operations in Al Nasiriyah Heart Center

Hussein Togun 1,* , Munaf Ahmed 2, Mohammed Hussein Haider 3, Tabarak Shaheed Ibrahim 4, Adyan Farhan Youssef 5
, Munaf Ahmed 2, Mohammed Hussein Haider 3, Tabarak Shaheed Ibrahim 4, Adyan Farhan Youssef 5
1 Department of Biomedical Engineering, University of Thi-Qar, 64001 Nassiriya, Iraq
2 Al-Nasiriyah Heart Center Thi-Qar, 64001 Nassiriya, Iraq
3 Department of Biomedical Engineering, University of Thi-Qar, 64001 Nassiriya, Iraq
4 Department of Biomedical Engineering, University of Thi-Qar, 64001 Nassiriya, Iraq
5 Department of Biomedical Engineering, University of Thi-Qar, 64001 Nassiriya, Iraq
* Corresponding authors: *[email protected], [email protected]
Available from: http://dx.doi.org/10.21931/RB/2023.08.02.50
ABSTRACT
The size and function of mechanical heart valves were evaluated in this article. The pathological cases that produce valve damage and lead to the most well-known rheumatic illnesses have been investigated. They induce stenosis and regurgitation of the valve, whether aortic or mitral, and other diseases, such as degenerative, congenital, and calcific valves. These cases occurred between 2015 and 2020, and the following are the most relevant characteristics include; patient's age, height, weight, kind of operation, cause, valve size, illnesses before the operation, complications after the procedure, cross-clamp time, Ejection Fraction (EF), and New York Heart Association (NYHA) before and after the operation. All were collected from the database. Because the valve size is directly and mainly connected to the surface area, the patient's height and weight were used to extract the surface area and correlate it to the valve size. It was also noticed that the mitral valve is more significant than the aortic valve because it is more profound than the aorta. The mitral valve was the most often replaced (51%), followed by the aortic valve (31%) and the double valve (18 %). The number of patients who have a valve replacement procedure fluctuates yearly, depending on the severity of the damaged valve. In some instances, the valve might be fixed without needing a replacement. Despite the difficulties of the procedure, there are relatively few deaths, and the data show that there are only two deaths in five years due to heart failure during the operation and cerebrovascular accidents.
Keywords: Mechanical Heart Valve; Mitral Regurgitation; Aortic Stenosis; Tricuspid Stenosis
INTRODUCTION
One or more of the heart's valves doesn't function appropriately in heart valve disease. The four valves in the heart keep blood flowing in the proper direction. One or more of the valves may not open or close correctly in some situations. Blood flow from the heart to the body may be disturbed due to this.
Adult echocardiography can detect mitral regurgitation (MR), the most frequently acquired valvular illness. Their onset can be sudden or chronic, and any condition that changes the structure of the mitral valve gear might be the cause 1. The primary MR is caused by defects in the mitral valve's components, whereas the secondary MR is caused by removing the neighboring ventricle and left atrium. Mitral valve asymmetry is caused by a leaflet lesion (e.g., mucinous degeneration, rheumatic regression or calcification, perforation), a sub valvular device (e.g., a stretched, loosened, or constricted tendon), and/or the mitral valve annulus being injured in primary MR (For instance, the mitral valve throat may be calcified, remodeled, or separated). A secondary ventricle or atrial mechanism can be seen in secondary MR. Dilation of the left ventricle and spherical remodeling damage the asymmetry of the mitral valve leaflet in secondary ventricular MR, displacing the papillary muscle that joins the chordates and envelopes the valve leaflet.
After coronary artery disease and systemic arterial hypertension, aortic stenosis is one of the most widespread and significant valve disease concerns. The aortic valve constricts as the illness progresses, limiting its open and closed capacity. Aortic stenosis, or AS, is a condition in which blood flow through the left ventricle is restricted. Aortic stenosis and its treatment have evolved throughout time. Rheumatic heart disease is replaced by calcific aortic valve disease, and echo is replaced by cardia.
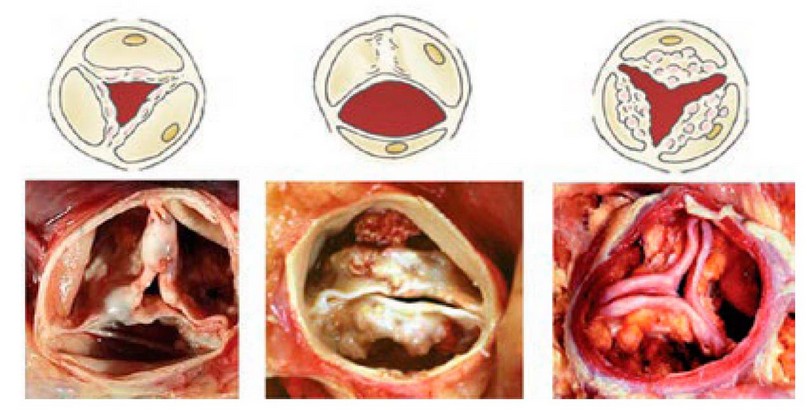
Figure 1: Etiologies of aortic stenosis 5.
Aortic regurgitation (AR): Rheumatic fever is among the most prevalent causes of aortic regurgitation in developing countries. It is caused by aortic valve malfunction due to aortic root and/or proximal ascending aorta anomalies.
Rheumatic fever, which a lumpy processor in the neck causes, is the most prevalent cause of tricuspid valve constriction. Although uncommon, tricuspid constriction can occur during fetal growth, congenital cardiac disease, tumors, or connective tissue disorders. A transthoracic echocardiogram TTE is required to diagnose and characterize Tricuspid Stenosis since it is frequently missed during a bedside examination. In most cases, TS is accompanied by TR. When the thickness and calcification of the valve and/or tendon are obvious, further signs of severe TS include mean pressure gradient >5 mmHg, pressure half-time ≥190 ms, valve area ≤1.0 cm2 (by the continuity equation), and right atrium and inferior vena cava IVC hypertrophy.
Aortic or mitral valvular disease affects almost 15 million people in the United States. Valve replacement surgery reduces morbidity and death in individuals with severe and symptomatic valvular heart disease. In the United States, 90,000 valve replacement procedures were conducted in 2009. Mechanical and bioprosthetic valves are the two types of replacement valves available.
The two most prevalent forms of mechanical valves, tilting-disc and bileaflet valves (Fig. 2), are both durable and need lifelong anticoagulation medication due to their thrombotic risk 9.
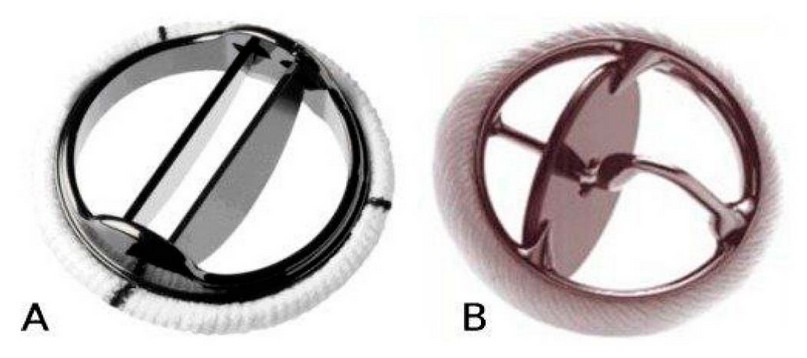
Figure 2. Images of some of the most popular prosthetic valves. A: leaflet-tilting-disk, B: single tilting-disk valve 10.
Some preparations required before and after heart valve surgery are shown in the Flow chart:
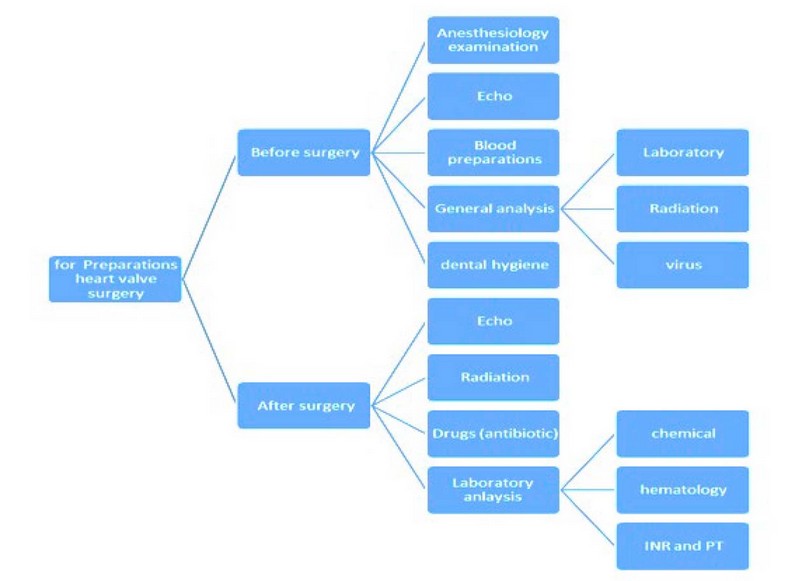
Figure 3. Flow chart Preparations before and after heart valve surgery flowchart.
MATERIALS AND METHODS
The results were studied at Nasiriyah Heart Canter, and the number of cases studied or worked on was 126, from 11–90 years. Several standards or criteria have been adopted, such as [ age, height, weight, EF, NYHA, time cross-clamp, complications, type of valve operation and the reason. The relationships that were built between:
1. Surface body area (SBA) and mechanical valve size.
2. EF and NYHA before and after the operation.
3. Type of mechanical valve replacement and number of patients.
4. Patient's age and number of cases.
5. Relationship between the operation time and type of operation.
When visiting the Al-Nasiriyah heart center, preparations are required before and after heart valve surgery. Before the surgery, the patient needs general analysis, including laboratory, radiation and virus analysis. Also, dental hygiene, because teeth are always the source of bacteria when they attack valves, they can't get out because the valve has no blood supply; thus, even when we give antibiotics, they can't reach the valve, so the valve must be replaced. Anesthesiology examination includes the function of the lung also laboratory, chemical and biology examination. Blood preparation includes fresh blood, donors who are identical to the patients, or whole banked, which mean the blood is kept (cold blood) in addition to blood product like plasma and platelet because, in some cases, we need just plasma or platelet, not the blood.
In addition to other analytical devices used for performing different analytical tests for patients, the device used for diagnosing heart diseases is the Echocardiogram device. This device is used to make a sonogram of the heart (using sound waves to produce heart images). Besides, depending on the information the doctor needs, the patient may have one of the following kinds of echocardiograms:
• Transthoracic echocardiogram
• Transesophageal echocardiogram
• Doppler echocardiogram
• Stress echocardiogram
In addition, in some cases, diagnostic catheterization is performed, and diagnostic procedures are performed using CT scans and MRIs. The treatment is performed by replacing the diseased valve or repairing it. The repair of diseased heart valves is performed for patients under 12 years old because if the valve in these ages is replaced, it's needed another replacement surgery in the future since the diameter of the valve changes as the patient continues to grow, except in complicated cases that's need to replace the diseased valves. For patients over 12 years old, a replacement surgery by mechanical or tissue valve is performed. A mechanical valve is made of mechanical parts that are tolerated well by the body, are more efficient, and remain more extended than a bioprosthetic valve (tissue valve). So, since it remains for approximately 10 years, the tissue valve is used only for patients over 75 years old. In Nasiriyah Heart Center, only mechanical valves are used by ST Jude Medical Company and Sorin Group.
The St. Jude heart valve, as shown in Fig (4A), was the first bileaflet mechanical heart valve. This bileaflet mechanical heart valve is designed and manufactured entirely from pyrolytic carbon. While the swing cuff is made from double-velour Dacron. Figure 4B shows St Jude's mechanical heart valve measurement.
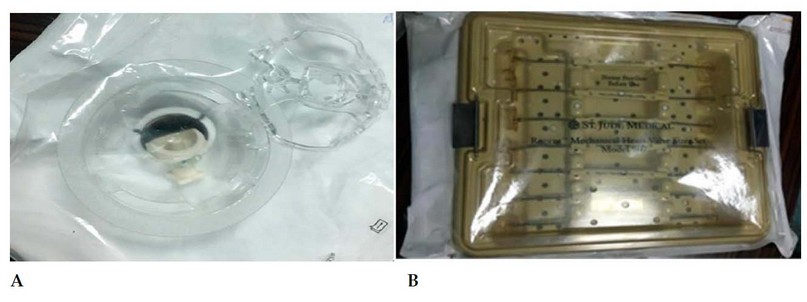
Figure 4. A. St-Jude mechanical heart valve. B. St Jude mechanical heart valve measurement tools
Fig (5A) and Fig (5B), they are showing the Sorin Group Mechanical Heart Valve that's also made from pyrolytic carbon and with carbon film coating and Sorin mechanical heart valve measurement.
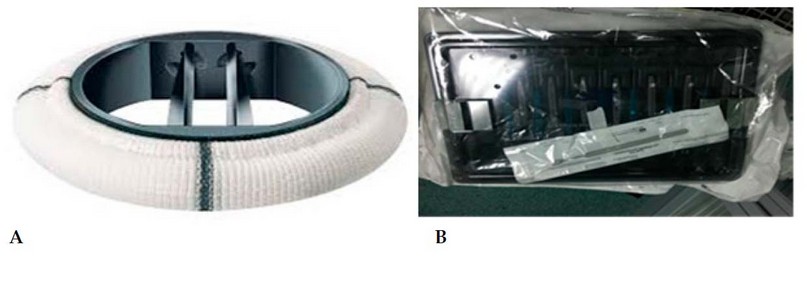
Figure 5. A. Sorin mechanical heart valve. B. Sorin mechanical heart valve measurement tools.
The patient's condition must be known. Laboratory examination includes chemical, hematology, Prothrombin Time (PT) and International Normalized Ratio (INR) examinations necessary for valve conditions, especially mechanical valves. The INR for the mitral valve is (2-2.5), for the aortic valve is (1.5-2) and for double valve replacement, it is (2.5-3.5); noticed that the aortic valve has the lowest ratio because the velocity in aortic valve is faster than the velocity in the mitral valve so the prothrombin will be less and is hard to produce. That means the supply pressure at the aortic valve is 120 mmHg and at the mitral valve is less than 10 mmHg. Also, radiation examination and medications are given to the patient, especially the antibiotic and warfarin.
RESULTS
In this article, the results covered 126 patients aged from 11 to 90 years old who underwent valve replacement between 2015 and 2020.
The number of cases and types of valve replacement surgery
Generally, there are three surgeries for heart valve replacement:
MVR: is a cardiac surgery that is performed when there is a regurgitation caused. In addition to that, there is stenosis. This led to replacing the MV with a mechanical or bioprosthetic valve.
AVR is a cardiac surgery performed when the diseased aortic valve is replaced by a mechanical or bioprosthetic valve when stenosis is caused or regurgitated.
Double valve replacement (DVR): is a cardiac surgical procedure in which a patient's diseased AV and MV are replaced with prosthetic valves.
The variation between the number of cases and types of valve replacement surgery is presented in Figure 6. From 126 cases, the mitral valve was the most has been replaced in 64 cases (51%), while the aortic valve replaced in 39 cases (31%), and the double valve was replaced in 23 cases (18%).
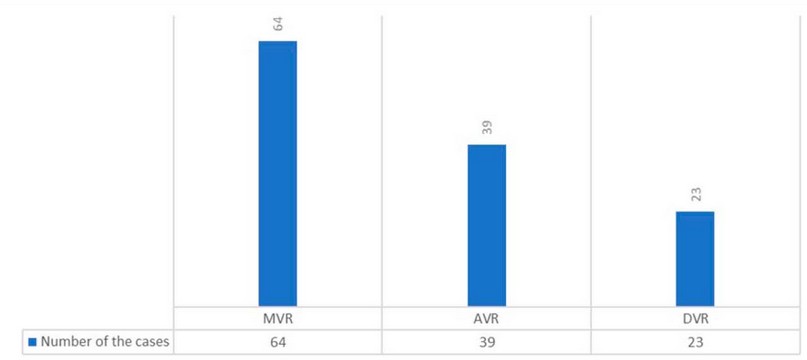
Figure 6. Variations between the number of cases and types of valve replacement surgery.
Number of cases and period time from 2015 to 2020
The number of cases in 2015 was 16 (13%), in 2016 was 22 (17%), in 2017 was 24 (19%), in 2018 was 25 (20%), in 2019 was 25 (20%), and in 2020 was 14 (11%). The results revealed that the maximum number of cases was 25 between 2018 and 2019, while the minimum was 14 through 2020. From the presented results, the number of cases increased through 2015- 2018 while decreasing through 2019-2020. The increase and decrease are because the number of cases depends on the number of patients who come to the Center. The previous findings are represented in Figure 7.
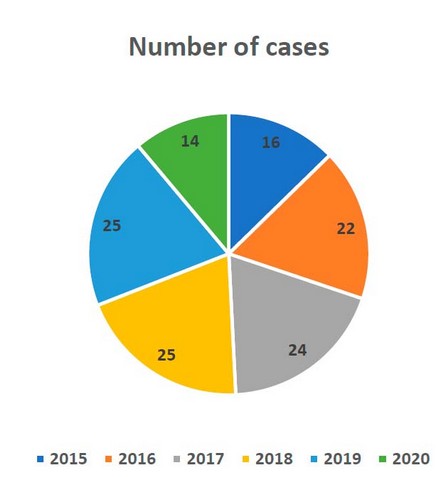
Figure 7. Number of the cases and period time from 2015 to 2020
Patients aged from 11 to 90 years
The results presented in Figure 8 covered patients aged from 11 to 80 years. The patients aged between 11 to 20 were 12 cases (9.5%), from 21 to 30 were 7 (5.5%), from 31 to 40 were 17 (13.4%), from 41 to 50 were 33 (26.19%), from 51 to 60 were 32 (25.3%), from 61 to 70 were 18 (14.28%), while cases 70, 72 and 76 were 5 (4.7%), but in 80's age only one case found (0.79%). The higher number of patients who underwent heart valve replacement was 27 for ages 41 to 50 years because the valve will be more active at this age. In addition, due to lack of attention and health care to prevent and avoid heart valve causes that will lead to damage and diseases thus at the end, the damaged heart valve must be replaced. At the same time, the lowest number was 1 for aged between 81 to 90 years.
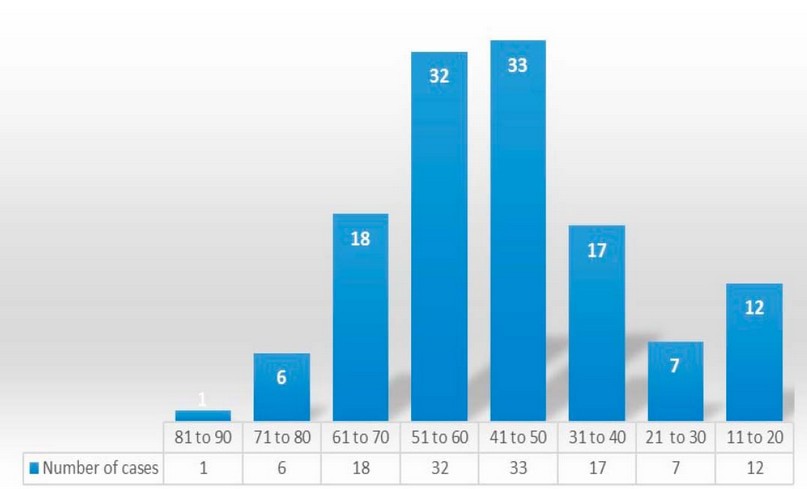
Figure 8. Variations between the number of cases and their age.
Mechanical heart valve size depending on surface body area (SBA):
The results presented in Figure 9 covered the relationship between mechanical heart valve size and the surface area where the result was calculated. The patient's height and weight were to extract the surface area and link it with the valve size, as it is directly and primarily related to the surface area. Also, valve size depends on the operation type in terms of whether it was a mitral or aortic valve, where the size of the mitral valve was always more significant than the aortic valve. The large size was used for mitral regurgitation, and the smaller was for aortic valve stenosis. Figure 9 covered 14 cases as examples of the relationship

Figure 9. Relationship between the size and SBA
Relationship between EF and NYHA
The result extracted for EF and NYHA before and after the operation because EF gives the doctor signals or clues about the condition of the patient's heart. NYHA is the primary measurement to determine the patient's heart condition, certified by the New York Heart Association according to the table of standards shown in Table 1. Important note NYHA depends on EF significantly. Figures 11 and 12 show the relationship before and after the operation.
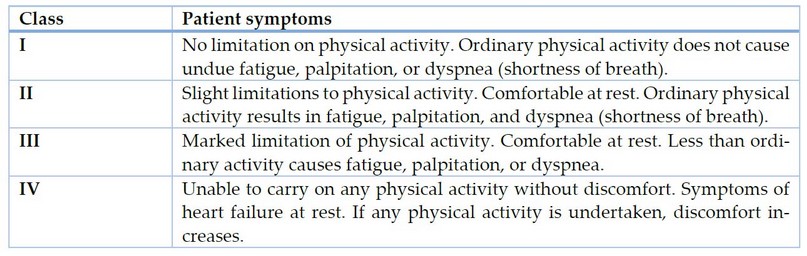
Table 1. NYHA standards
Class
Patient symptoms
I
No limitation on physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, or dyspnea (shortness of breath).
II
Slight limitations to physical activity. Comfortable at rest. Ordinary physical activity results in fatigue, palpitation, and dyspnea (shortness of breath).
III
Marked limitation of physical activity. Comfortable at rest. Less than ordinary activity causes fatigue, palpitation, or dyspnea.
IV
Unable to carry on any physical activity without discomfort. Symptoms of heart failure at rest. If any physical activity is undertaken, discomfort increases.
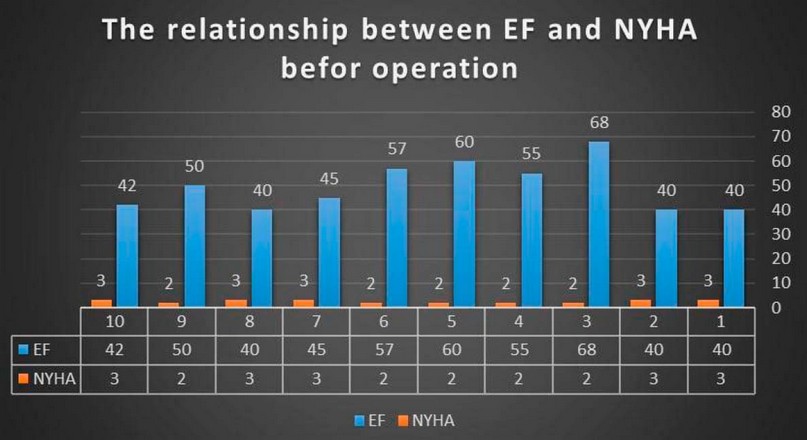
Figure 10. EF, NYHA before operation.
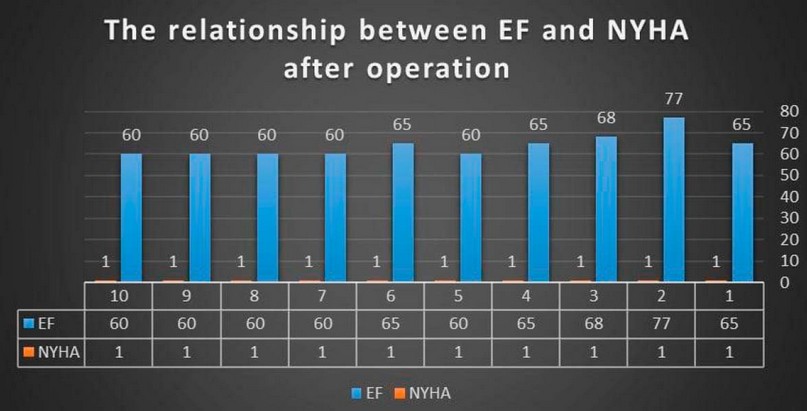
Figure 11. EF, NYHA, after the operation.
Mortality from 2015 to 2020
The total center mortality from 2015 to 2020 presented in the Figure 13 where was just two cases, in 17 February 2015 patient underwent to AVR surgery at age 41 years old died because of cerebrovascular accident (CVA). In 27 December 2020 patient underwent to DVR surgery at age of 55 years old and died because of heart failure.
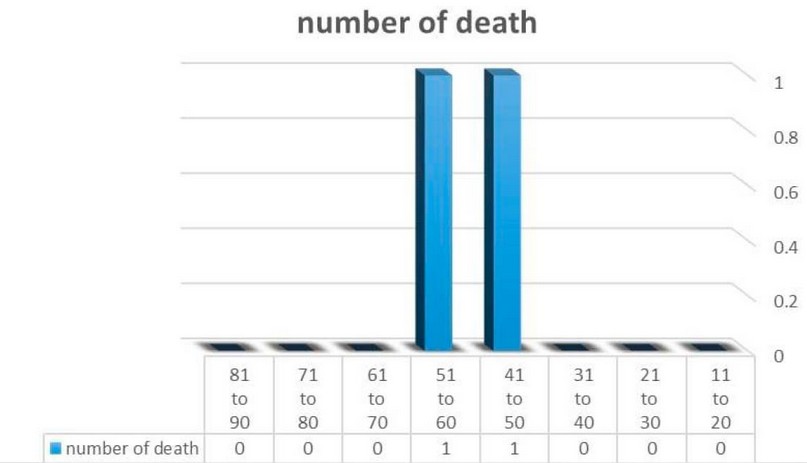
Figure 12. The number of deaths for patients who underwent heart valve replacement.
Relationship between the operation time and type of operation
The results showed that the operation time depends on the operation type performed. However, in the last five years, the operation time has become less than the previous years due to the development of expertise and equipment. However, the results showed that the time required to perform DVR is much more than the time required to replace the MV or AV. Moreover, the complications are related to the time of the operation, as the longer the operation, the greater the complications. Figure 14 shows the relationship between the operation time and the type of operation.
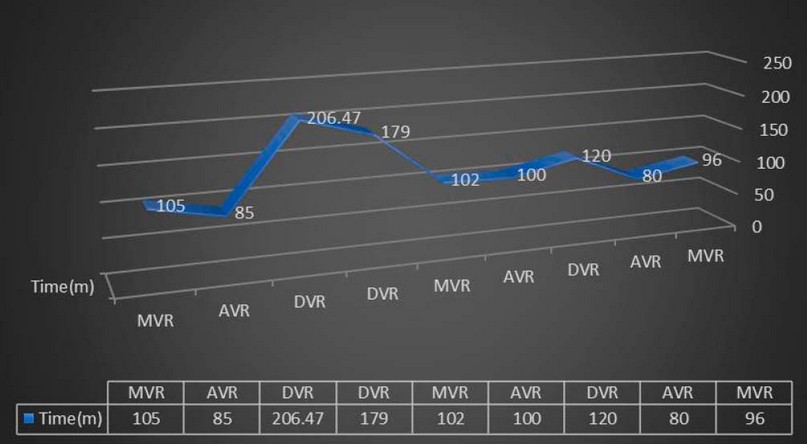
Figure 13. Relationship between the operation time and type of operation.
.
DISCUSSION
A decrease in left ventricular contraction results in a decrease in papillary muscle contractility, which leads to a decrease in throat surface subsidence and leaf acclimation 2. Moreover, transcatheter aortic valve replacement for aortic valve implantation (TAVI) aortic valve replacement is the procedure of choice for diagnosing and tracking aortic stenosis. However, because medication treatment has not been proven to help lower valve stenosis, surgery remains an option for TAVI in surgical (SAVR) or dangerous instances5. However, the prevalence of AR is expected to be 4.9 percent for moderate aortic regurgitation and.5 percent for severe aortic valve regurgitation, according to the Framingham research 6. AR is a significant valve insufficiency or chronic valvular disease produced by a serious etiology. Presentation, etiology, direction, and natural history are all different 7. Transcatheter mitral valve-in-valve (TMVIV) or valve-in-ring (TMVIR) surgery presents an alternative approach for high-risk patients, according to 3. They concentrated on the TMVIV and TMVIR procedures operational and postoperative outcomes.
Furthermore, 4 conducted a comprehensive review and meta-analysis on mitral valve repair and replacement in severe ischemic mitral regurgitation. They discovered that the RPR arm tended to improve perioperative survival. Furthermore, transdermal treatment for severe isolated symptomatic TS without TR is very unusual. Recognizing its short-term limitations and lack of evidence on long-term results, balloon tricuspid valve incision may be explored 8.
CONCLUSIONS
The pathological cases that cause valve damage and that lead to the most famous rheumatic diseases have been studied, as they cause stenosis as well as regurgitation of the valve, whether aortic or mitral, in addition to other diseases such as degenerative, congenital and calcific valve. These cases were in the years between 2015-2020. The most important points extracted from these results are: The extracted results were (patient's age, height, weight, type of operation, the reason for the operation, valve size, symptoms before the operation, complications after the operation, the cross-clamp time, EF and NYHA before and after the operation).
The percentage of patients who underwent a valve replacement operation varies yearly, according to the damaged valve's need for replacement. Sometimes, the valve was repaired without the need for a replacement operation. Also, the increase and decrease are because the number of cases depends on the number of patients who come to the Center. This depends on the patient's culture, as some patients fear operating because of a delay in examining such cases.
The mitral valve was the most has been replaced in (51%), while the aortic valve was replaced in (31%) and the double valve was replaced in (%18). It was also noted that the size of the mitral valve is larger than that of the aortic valve because the mitral is more profound and significant than the aortic valve. Moreover, this valve is one of the most critical valves of the heart, as it transports oxygen-laden blood from the lungs to the heart and then pumps it to the rest of the body.
It was noted that the highest percentage of valve replacements was from 41-50. This is because at this range it is the average human life span and increased exposure to heart disease risk factors (such as obesity, diabetes, smoking, and high blood pressure), while the lowest percentage was from 81-90, where at this age the replacement operations were only one.
The patient's height and weight were to extract the surface body area and link it with the valve size. Where the size directly and largely depends on the surface body area and on type of the valve, and the size of valve differential between the standard valve and mechanical valve (for SBA (2) normal mitral valve:24.2 while mechanical mitral valve: 31) the size was more significant in mechanical because dealing with a foreign body is vulnerable to blood pooling and causing a clot.
The most critical and challenging replacement operations were for patients with rheumatic and dual valves, where two valves are placed for them due to the presence of stenosis and regurgitation, which may be in the aortic or mitral valve, which takes time and causes significant and many complications.
The patient's height and weight were to extract the surface body area and link it with the valve size, as it is directly and primarily related to the surface area.
The EF was extracted before and after the operation to monitor the patient's condition and the degree of improvement. As for the NYHA, it was the main measure to determine the patient's condition, as it relied on the EF and the patient's condition (complications).
There are very few deaths in such an operation, despite its difficulty. Still, it was found from the results that in five years, there are only two deaths due to heart failure during the operation and cerebrovascular accident.
Author Contributions: Hussein Togun and Munaf Ahmed conceived the presented idea. Hussein Togun developed the theory and performed the computations. Mohammed Hussein Haider, Tabarak Shaheed Ibrahim and Adyan Farhan Youssef collected data and verified the analytical methods. . All authors discussed the results and contributed to the final manuscript.
Data Availability Statement: Nasiriyah Heart Center is a medical center in Nasiriyah, Dhi Qar Governorate, Iraq, specializing in diagnosing and treating heart diseases such as ischemic heart disease, congenital heart defects, and valvular heart defects. The Center was opened on 10 July 2007. It employs a specialized staff of doctors, engineers and specialized medical and technical staff. The Nasiriyah Heart Center, consider the first place in southern Iraq in this rare specialty, is also an important step in the transfer of strategic projects from the capital to the rest of the regions to provide medical and treatment services for heart patients in Dhi Qar Governorate and other governorates.
REFERENCES
1. Dal-Bianco JP, Beaudoin J, Levine RA. Basic mechanisms of mitral regurgitation. Can J Cardiol. 2014;30(9):971–81. https://doi.org/10.1016/j.cjca.2014.06.022.
2. Carpentier A, Adams DH, Filsoufi F. Carpentier's reconstructive valve surgery. from valve analysis to valve reconstruction. Philadelphia: Saunders Elsevier; 2010.
3. Tamer Owais, Mohammad El Garhy, Sebastian Elvinger, Eva Harmel , Tatiana Maria Sequeria Gross, Harald Lapp, Thomas Kuntze, Wolfgang Von Scheid, Evaldas Girdauskas , Mahmoud Al‑Jassem and Philipp Lauten, Contemporary results of transcatheter mitral valve procedures: bi-centric retrospective analysis. The Egyptian Heart Journal, 2022; 74:19.
4. Mohamed A Gamal , Mohamed M El-Fiky , Mahmoud M Gamea , Ihab Ali, Mitral valve repair versus replacement in severe ischemic mitral regurgitation systematic review and meta-analysis, J Card Surg. 2022 Jun;37(6):1591-1598
5. Lindman BR, Clavel MA, Mathieu P, Iung B, Lancellotti P, Otto CM, Pibarot P. Calcific aortic ste nosis. Nat Rev Dis Primers. 2016; 2:16006
6. Singh JP, Evans JC, Levy D, Larson MG, Freed LA, Fuller DL, Lehman B, Benjamin EJ. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study). Am J Cardiol. 1999;83(6):897 902
7. Iung B, Baron G, Butchart EG, Delahaye F, Gohlke Bärwolf C, Levang OW, Tornos P, Vanoverschelde JL,ermeer F, Boersma E, Ravaud P, Vahanian A. A pro spective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24(13):1231–43
8. Lin FY, Devereux RB, Roman MJ, Meng J, Jow VM, Simprini L, Jacobs A, Weinsaft JW, Shaw LJ, Berman DS, Callister TQ, Min JK. The right sided great ves sels by cardiac multidetector computed tomography: normative reference values among healthy adults free of cardiopulmonary disease, hypertension, and obesity. Acad Radiol. 2009; 16:981–7
9. Z. Al-Fayyadh, D. .; Hasson, A. A. .; Hussein, A. K. .; Hassan, R. K. Effect Of Humic Acid Spray On Growth Characteristics Of Wheat Varieties . Journal of Life Science and Applied Research. 2020, 1, 10-19..
10. Alkubaisy,S.A., A.A. Majid, S.M. Abdulateef, F.A. Al-Bazy, O.K. Attallah, O.M. Abdualmajeed, Th. T. Mohammed, F.M. Abdulateef, K.I. Mahmud. Effects of In-Ovo injection of Biotin on chick's embryonic development and physiological traits. IOP Conference Series: Earth and Environmental Science, 2021; 761(1), 012111.
Received: May 15 2023/ Accepted: June 10 2023 / Published:15 June 2023
Citation: Togun, H.; Ahmed, M.; Haider, M.H.; Ibrahim, T.S.; Youssef, A.F. Evaluation study the size and function of mechanical heart valve replacement operations in Al Nasiriyah Heart Center. Revis Bionatura 2023;8 (2) 50. http://dx.doi.org/10.21931/RB/2023.08.02.50