2022.07.02.15
Files > Volume 7 > Vol 7 No 2 2022
Determination of cumulative glucose levels HbA1C and some biochemical variables in the serum of Diabetic nephropathy patients

Eman S. AL-sofi1, Huda Y . AL-Attar 2
1,2University of Mosul, College of Science, Department of Biology. Iraq
Correspond Author: [email protected],
Available from: http://dx.doi.org/10.21931/RB/2022.07.02.15
ABSTRACT
The study included measuring the concentrations of each of the cumulative sugar HbA1C Glycosylated hemoglobin, urea, creatinine, uric acid, glucose, glucose uric acid, albumin, total protein and calcium, in addition to identifying the concentrations of some electrolytes (sodium, potassium, chloride, calcium) in (35) blood samples from patients with diabetic nephropathy (14 males, 12 females) aged (16-62) years who came to some laboratories in the city of Mosul and compared them to control samples (26) samples. The results showed a significant increase in cumulative sugar, uric acid, glucose and potassium concentrations in the serum of patients of both sexes. An insignificant increase in urea and creatinine concentrations and a significant decrease in albumin, sodium and chloride concentrations, while calcium and total protein did not show a significant difference compared to control samples. When comparing cases of infection between males and females, the results showed a significant increase in the cumulative sugar level for males and an insignificant increase in glucose concentration. In contrast, creatinine, uric acid, total protein and albumin did not significantly differ for males compared to infected females.
Keywords cumulative glucose, biochemical variables, Diabetic
INTRODUCTION
Diabetic neuropathy is one of the most common complications of diabetes, which affects a third of patients with type 2 diabetes1, and is characterized by the occurrence of many pathological severe changes that may lead to death, and about 40% of these patients eventually develop kidney disease2 compared to other causes of kidney failure.
The increase in the concentration of sugar in the blood is the main factor for diabetic nephropathy because it affects the physiological functions of the kidneys and leads to their damage. In addition to other factors that contribute to the infection, including genetic predisposition, high blood pressure and atherosclerosis3 Capillary damage occur in diabetic nephropathy, which leads to protein loss through diuresis, a decrease in the filtering activity of the renal glomerulus, and an increased risk of death from heart and blood vessels disease4,5.
The illness affects the efficiency of the kidneys in removing toxins and excreting excess fluids from the body and thus their accumulation in the blood6 and symptoms of morbidity appear after ten years in diabetics (type 1). However, symptoms appear quickly in diabetics (type 2) and are represented by high blood pressure, increased cholesterol concentration, swelling of the feet, loss of appetite, fatigue and nausea7,1 Research has indicated that patients with type 1 diabetes develop symptoms similar to those of the end-stage kidney deficit early compared to patients with type 2 diabetes8,9. Many tests are considered guides to indicate kidney function and detect morbidity in diabetic patients, including measuring the concentration of urea, creatinine, uric acid, total protein, albumin and sugar, and cumulative sugar10.
Hemoglobin glucose (cumulative sugar) HbAIC is one of the essential proteins associated with red blood cells 11 as its level increases with the increase in the concentration of glucose in the blood, and this measurement is used to determine the concentration of glucose in the blood for the previous three months 9, which helps to maintain blood sugar. Blood glucose level is used to assess metabolic changes during treatment 3.
Urea is synthesized in the liver and is one of the pathways for protein breakdown into amino acids. The level of urea represents the amount of protein that is consumed and excreted by the kidneys12 A defect in the filtering activity of the renal glomerulus leads to a change in the concentration of urea in blood, as well as the condition in cardiovascular diseases and liver diseases13 As for creatinine test, it is more accurate, and its concentration is affected by age and weight, this changes the efficiency of the glomerular filtration and increases its concentration in cases of renal failure and urinary retention3 Another test that falls within the determination of kidney functions is uric acid, whose concentration is controlled by many factors such as heredity, high blood pressure, diabetes and bone diseases, which affect the efficiency of the kidneys, and consequently to the formation of stones and possibly to renal failure14.
Tests for protein are indicators of kidney, liver, and bowel disease3. In addition to the seventh variable, electrolytes are among the essential elements inside and outside cells, including fluids and blood. Calcium is a necessary element for the body, and the potassium test helps diagnose diseases of the bones, heart, nerves and kidneys. At the same time, magnesium has an essential role in diagnosing diseases. Disorders of the nervous system, muscles and kidney efficiency, as well as its role in the transport of calcium and potassium, as well as sodium, have a role in maintaining osmotic pressure and are considered a guide in diagnosing kidney diseases and estimating chloride concentrations has a role in determining renal diseases and adrenal gland functions15,13.
To determine the effect of cumulative sugar level and biochemical variables on diabetic patients, this study discovered the serum concentrations in diabetics patients of both types who suffer from renal impairment.
MATERIALS AND METHODS
The blood samples were collected from (35) patients (14 males, 12 females) of different ages ranging from (16-62) years who arrived at some laboratories in the city of Mosul, as well as (26) blood samples were collected from healthy people of the same age groups. The following tests were performed on the blood serum: Measuring the cumulative glucose level HbA1C Multimeter (AFIAS) Korea-Boditech Corporation. Using an AFIAS device and measuring urea concentration Urea in Switzerland-AGAPPE and Measuring creatinine concentration creatinine, total protein, albumin, Elements (CI-, K+, Na+) by France-BIOLABO kit and Concentration measurement Uric Acid, Glucose, Calcium Ca+ in several sizes Spain-Linear.
Statistical analysis
The results were statistically analyzed, using a test t-test to show the difference between two groups at the level of significance (α = 0.05), as well as finding the linear correlation coefficient to find the relationship between biochemical variables, HbA1C and Creatinine at the level of significance (α = 0.05, α = 0.01), with finding the coefficient of determination to show the effect of age on the change in HbA1C, in addition to finding the significance of the relationship between them through the ANOVA table16.
RESULTS AND DISCUSSION
The results of table (1) showed a significant increase in the concentrations of cumulative sugar, HbA1c, uric acid and glucose in the patients' serum compared to the control groups and a non-significant decrease in the concentrations of urea and creatinine; the reason for the increase in the cumulative sugar level may be due to damage to the blood vessels17. When glucose concentrations rise, glucose molecules stick to molecules of proteins and platelets, and this leads to disruption of their function as a result of protein molecules sticking together; this narrows the diameter of the arteries and thus reduces the amount of oxygen that reaches the tissues, so high levels of HbAIC lead to great risks of cardiovascular disease Hematologic and stroke18.19.
The increase in urea and creatinine levels is due to the rise in sugar levels as a result of insulin secretion disturbance20, nephropathy that leads to arterial hypertension and a defect in its physiology, and the cause of high creatinine concentration may be urinary retention that leads to renal failure as a result of a defect in the filtering activity of the renal glomeruli10, which leads to an increase in it in the blood, and is accompanied by the deposition of uric acid forming kidney stones in case it is higher than the normal level15. The high concentration of glucose in the blood affects the nerves of the kidney nephrons over time10.
The results of table (1) showed a significant decrease in albumin and electrolytes (sodium and chloride) in patients of both sexes compared to the control groups. This is due to the large quantities of albumin excreted daily in this type of patient and for both types (first and second), which causes kidney damage and then cardiovascular complications3. And the reason for the decrease in chloride and sodium is due to the significant correlation between these two elements and the fact that the volume of extracellular water decreases, the state of respiratory acidosis and the slowness of metabolic processes, and this causes renal impairment21,6.
Calcium and total protein did not significantly differ in both sexes compared to the control groups, unlike potassium, as it showed a significant increase. The reason may be its effect on the concentration of hormones, including insulin and thyroid hormones.17,22.
To show the effect of the sex factor on the variable's concentrations, the results of table (2) showed a significant increase in the concentration of cumulative sugar and glucose and an insignificant rise in both the concentration of urea and creatinine in the serum of both males and females compared to the control groups, but it was found that there was a significant increase in the concentration of uric acid in females than in males and this is as a result of metabolic disorder, especially after menopause and the change in the level of hormones19,17, and a significant decrease in the concentration of total protein and chloride in the blood serum of both sexes was shown. The reason is mainly due to the presence of chloride in extracellular fluids, formation of respiratory acidosis and impaired renal function in regulating water balance23.
As for a reason for the decrease in total protein, it is due to the high glucose, which helps to get infections in the renal tissue and its damage, leading to the loss of large amounts of protein through urine. Accordingly, the concentration of protein in the serum is lower than the normal limits24.
The results of table (2) showed an insignificant decrease in the albumin concentration in males and a significant reduction in females compared to the control groups. The reason is attributed to the complications of diabetes, which leads to a defect in the function of the kidneys and the occurrence of cardiovascular complications, and thus the excretion of large amounts of protein through Urine15.
It is noteworthy from the same table that the calcium concentration did not show a significant difference in males, while it showed an insignificant decrease in females compared to the control groups. This is attributed to a defect in kidney function that leads to glomerular filtration disorder and vitamin D deficiency, which causes osteoporosis and osteoporosis25,17.
A significant decrease in sodium concentration was also observed in the serum of males and an increase in the serum of females compared to the control groups. The reason is fluid loss due to diarrhea and frequent urination of diabetic patients and the effect of renal impairment associated with diabetes mellitus. The increase in potassium concentration in both females and males is due to the disorder of the kidneys' functioning, its low filtering capacity, the acid-base imbalance that affects the concentration and the accompanying nephropathy and heart disease22.
To find the relationship between the concentration of the cumulative sugar level and the rest of the biochemical variables in diabetic nephropathy patients, according to the linear correlation coefficient, the results of table (3) showed a significant direct relationship between the cumulative sugar level and each of the concentrations of urea, creatinine, uric acid and glucose, and this is due to the direct relationship between glucose concentration and cumulative sugar26.
The table results also showed an insignificant inverse relationship between the cumulative sugar concentration and each of the total protein, albumin and elements (calcium, chloride, potassium, sodium).
The results of table (4) showed that there was a significant positive relationship between creatinine concentration and each of (HbA1C, urea, uric acid, glucose), the cause is due to diabetic nephropathy, and this is the main cause of chronic renal failure, so both urea and creatinine are good indicators that help determine kidney functions during nephropathy in patients with diabetes27 There was a significant inverse relationship between the concentration of creatinine and each of the total protein, albumin and elements (calcium, chloride, potassium and sodium).
The results of table (5) showed that there is a direct relationship between the cumulative sugar level HbA1C and age; according to the correlation coefficient and determination, the reason is due to increasing age, many physiological variables occur, such as a decrease in the function of the pancreatic islets, the sensitivity of tissues to insulin, the activity of insulin receptors, and in muscle tissues, glucose consumption gradually decreases in general, and the level of glucose increases with age28,29.
Through a table of variance analysis ANOVA The results of table (6) showed a significant effect of age on the level of HbA1C, which led to a decrease in the diagnostic efficiency of the level of HbA1C, as with age the number of RBCs decreases physiologically30 This leads to a decrease in bone marrow production, especially in the elderly, and a decrease in kidney function31 .
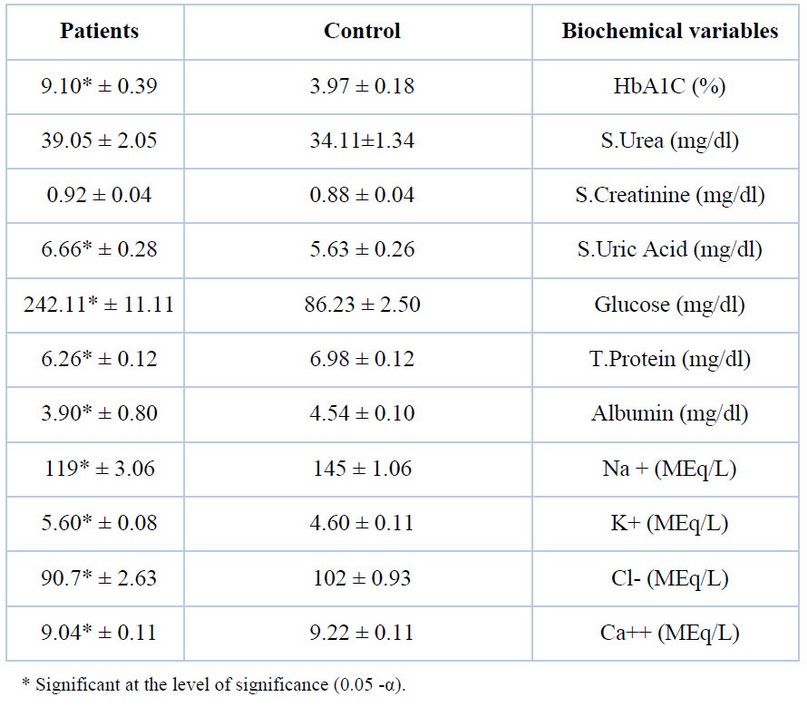
Table 1. Concentrations of variables in the blood serum of diabetic nephropathy patients compared to control groups Variable concentrations standard deviation ± average.
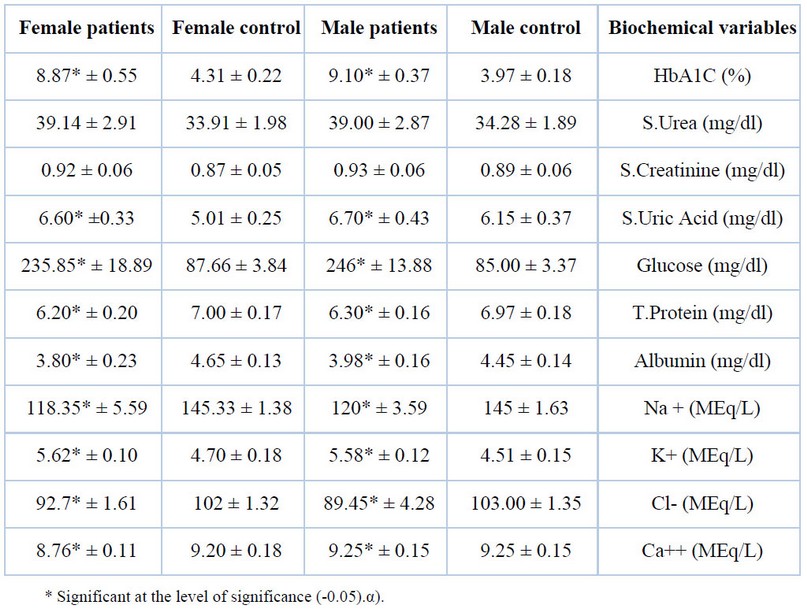
Table 2. Concentrations of biochemical variables in the blood serum of male and female patients compared to control groups standard deviation ± average
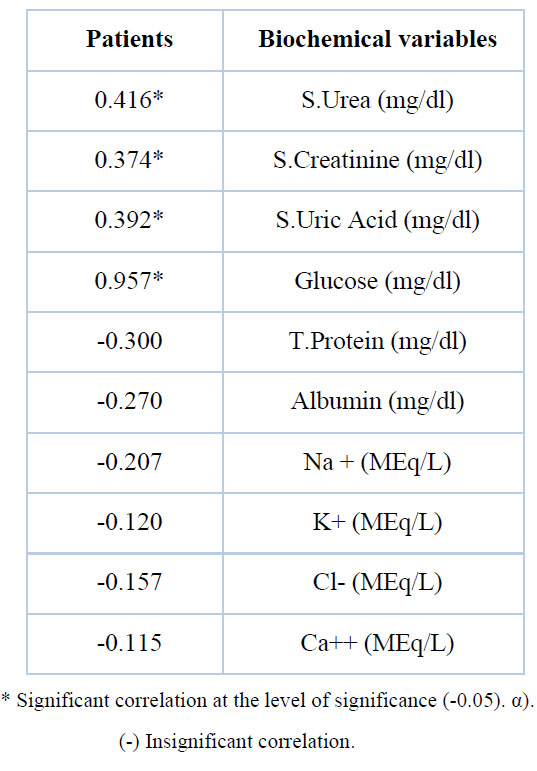
Table 3. The relationship between HbA1C and other biochemical parameters in patients with diabetic nephropathy

Table 4. the relationship between concentration creatinine and other biochemical parameters in patients with diabetic nephropathy
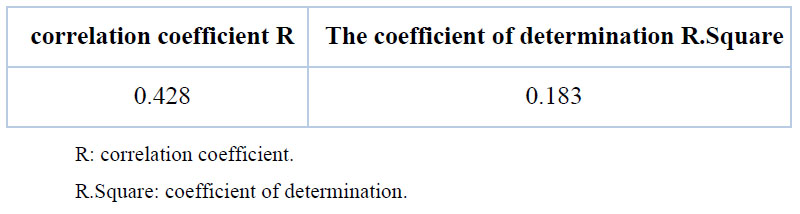
Table 5. correlation coefficient and determination to show the relationship between age and the value of HbA1C in patients
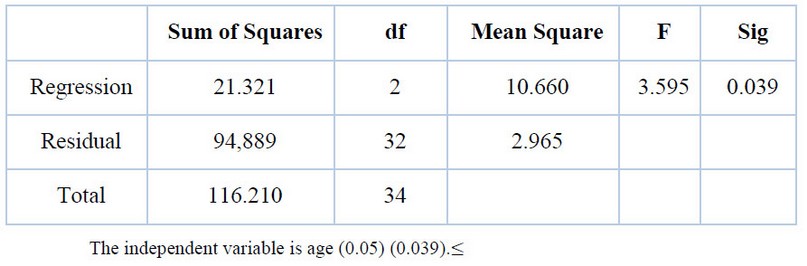
Table 6. shows the variance ANOVA to show the effect of age on HbA1C in patients
CONCLUSION
We conclude that there is an increase in the cumulative sugar level of the affected males compared to the control samples. With no significant difference for the other indicators, values for females, no significant difference was recorded.
Funding: self-funding
Acknowledgments: In this section, we acknowledge any person who supports us to complete this project.
Conflicts of Interest: there is no conflict
REFERENCE
1. Sulaiman, KM. ''Diabetic nephropathy: recent advances in pathophysiology and challenges in dietary management'', US national laboratory of medicine, national institute of health, V.2019؛ 11:7.
2. Umanath, K., Lewis, BJ. ''Update on diabetic nephropathy: Core curriculum 2018؛, AJKD Vol. 71, Iss. 6.
3. Mcfarlane, P., Cherney, D., Gilbert, RE, and Senior, P., . "Chronic kidney disease in diabetes", Can J diabetes, 2018؛ 42. S201-S209.
4. Sharaf Eldin, UAA, Salem, MM, Abdulazim, DO . ''Recent advances in management of diabetic nephropathy'', J. of clinical and experimental nephrology,2017؛ ISSN 2472-5056.
5. Yang, Z., Feng, L. Huang, Y. and Xia, N. ''A different diagnosis model for diabetic nephropathy and non-diabetic renal disease in patients with type 2 diabetes complicated with chronic kidney disease'' , J. diabetes, metabolic syndrome and obesity: Targets and therapy,2019؛ V. 12.
6. Subramanyam, SK, Gosavi, S. Tenneti, D., and Murgod, R., . "Evaluation of the role of HBA1C in chronic kidney disease", J. of clinical and diagnostic Research,2018؛ V. 12(7) : BC01-BC04.
7. Zhang, J., Liu, and Qin, X. ''Advances in early biomarkers of diabetic nephropathy'', Rev Assoc Bras;2018؛ 64(1): 85-92.
8. Zürbig, P., Mischak, H., Menn, J. and Haller, H., . "CKD273 Enabeps efficient prediction of diabetic nephropathy in nonalbuminuric patients", Diabetes care,2019؛ 42(1): e4-25.
9. Lee, YM, Huang, CJ, Chen, CS, Chiou, CYH, and Wu, YP. ''Association of HbA1C variability and renal progression in patients with type 2 diabetes with chronic kidney disease stages 3-4'', Int. J. Mol. Sci. 2018؛ 4116; doi: 10. 3390/ijms 19124116.
10. Chutani, A and Pande, S. "Correlation of serum creatinine and Urea with glycemic index and duration of diabetes in type 1 and type 2 diabetes mellitus: a comparative study." National journal of physiology, pharmacy and pharmacology.2017؛ Vol. (7), Issue (9).
11. Gutierrez, RR, Adame, LGM, Tamez, RT, Colmenero, ADG, Pacheco, SCR, Plazas, ESA, Santilana, KMS, Sarinana, GL, Nava, GV, Gonzalez, GG,. "Hypertrigly ceridemia and its associated study, HbA1C test: A prospective in Vivo controlled study," International journal of endocrinology,2019؛ Article ID 4784313, 6 Pages.
12. Kebar, MS, Sharagi, A., Bashardoust, B., Iran Parvar, M., Fekri, H., and Habib Zadeh, A. ''The therapeutric effect of sevelamer on blood sugar, HbA1C, Lipid, and hs-CRP in patient with diabetic nephropathy; A preliminary study'', J. nephropathol, 2018؛ 7(2): 65-68.
13. Al-Attaby, TKA, Al-Lami, DQM . "Role of Calcium-Regulating hormones, adipocytokines and renal fuction test in the progress of type 2 diabetes mellitus in sample of Iraqi patients", Iraqi journal of agricultural science,2019؛ 50 (1): 343-351.
14. Pavithra, V., Revathy, K., and Swaminathan, S. "Association between Uric acid and HbA1C in type 2 diabetes mellitus in comparison with controls", Int. J. Curr. Microbiol. App. Sci.2016؛ 5(4): 585-589.
15. Najeeb, Q., Aziz, R. and Hamid, S. "To evaluate the levels of glycat hemoglobin, Serum Calicum, Magnesium, Phosphate, Uric acid and microalbuminuria in patients with newly diagnosed type 2 diabetes mellitus". IntJ Res Mes Sci,2014؛ 2(4): 1462-1465, PISSN2320-6071 I eISSN 2320-6012.
16. Kikwood, BR. ''Essential of medical statistics, Balchwell scientific publications Oxford'',1988؛1st, pp. 43-56.
17. Kumar, A., Rageswari, KR, and Swaminathan,.''The diagnostic significance of Calcium Phosphorus, Magnesium and Uric acid in type 2 diabets mellitus and their association to HbA1C'', J. of chemical and pharmaceutical Research,2015؛ 7(8): 390-397, ISSN: 0975-7384.
18. Khorasani, E.,. ''Prevalence of peripheral neuropathy and its related factors in diabetic children, Neishabour city, Iran'', Int J pediatr,2018؛ Vol. 12, Serial No. 60.
19. Su, JB, Zhao, LH, Zhang, XL, Cai, H., L., Huang, HY, Xu, F., Chen, T., and Wang, Q., X., . "HbAIC variability and diabetes peripheral neuropathy in type 2 diabetes patients", US national library of medicine national institutes of health, 2018.
20. Nassrullhah, HAA, Al-Hialaly, KA, Al-Hadad, HS and Abutiheen, AAK,. "Changes in serum Potassium and serum creatinine in hypertensive patients treated with captopril with or without amlodipine", Kerbala journal of pharmaceutical science,2016؛ No. (11).
21. Al-Hassan, AMA, Hatif, AR, Dhari, HR and Edan, HE . ''Study on diabetes mellitus and the balance if electrolytes'', J. of Babylon university/Pure and applied sciences,2016؛ No. (7), Vol. (24).
22. Nagai, K., Ueda, S., Toshio, D., and Minakuchi, J. "Low serum sodium concentration is a prognostic factor related to current blood glucose level in stable hemodialysis patients: an observational study", Contributed equal renal replacement therapy, 2017؛ 20173: 55.
23. Fourkiotis, V., Vonend, O., Diederich, S., Fischer, E., Lang, K., Endres, S., Beuschlein, F., Willenberg, HS, Rump, CL, Allolio, B., and Reincke , M. "Effectiveness of eplerenone or spironolactone treatment in preserving renal function in primary aldosteronism", European journal of endocrinology,2013؛ 168.75-81.
24. Welsh, IG, Coward, JR. "The podocyte in diabetic nephropathy: recent advances", Diabetic nephropathy, 2018؛ pp 171-182.
25. Lim, ML, Kuo, TH, and Chen, CH,. ''Low serum Calcium in associated with poor renal outcomes in chronic kidney disease stages 3-4 patients'', BMC nephrol, 2014؛ 15: 183.
26. Sivasubramanian, V., Jetty, K., and Kumar, SS. "Correlation of HbA1C with urinary ACR, Serum creatinine and eGFR in type-2 diabetes mellitus at puducherry, south India", International journal of Research in medical sciences , 2019؛. 7, Issue 5, p. 1924.
27. Zubair, M., Malik, M., and Ahmed, J. ''Correlation of HbA1C and S. creatinine along with microbiological profiling of infected ulcers; cases of diabetic patients'', US national library of medicine national institute of health,2019؛ 13(1): 30-34.
28. Masuch, A., Friedrich, N., Roth, J. Nauck, M., Müller, AU and Petersman, A. ''Preventing misdiagnosis of diabetes in the elderly: Age-dependent HbA1C reference intervals derived from two population based study cohorts'', BMC endocrine disorders, 2019.
29. Cho, NY, Lee, OK, Jeong, J., Park, JH, Kim, MS, Shin, YH, Hong, MJ, Ahn, WC, and Choi, CY, . "The role of insulin resistance in diabetic neuropathy in Koreans with type 2 diabetes mellitus: A6-Yas Follow-Up study", YONSEI MED, 2014؛ J55(3): 700-708.
30. Ma, Q., Liu, H., Xiang, G., Shan, W., and Xing, W., . "Association between glycated hemoglobin A1C level with age and gender in Chinese adults with no prior diagnosis of diabetes mellitus", US national library of medicine, national institutes of health, 2016.
31. Wu, L.. ''Effect of age on the diagnostic efficiency of HbA1C for diabetes in a Chinese middle-aged and elderly population: the Shanghai changfeng study'', 2017؛ Plos one 12(9):
Received: 27 November 2021 / Accepted: 18 January 2022 / Published:15 May 2022
Citation: AL-sofi, Huda y . AL-Attar, Determination of cumulative glucose levels HbA1C and some biochemical variables in the serum of diabetic nephropathy patients. Revis Bionatura 2022;7(2) 15. http://dx.doi.org/10.21931/RB/2022.07.02.15