2023.08.03.93
Files > Volume 8 > Vol 8 No 3 2023
Differences between the responses of parents and teachers Anxiety screening for autistic children aged 3-5 years: a cross-sectional study

Vanessa Andreina Loor Robles1 , Karime Montes-Escobar2, Jimmy Manuel Zambrano Acosta1, Hipatia Meza Intriago1, Aline Siteneski3*
, Karime Montes-Escobar2, Jimmy Manuel Zambrano Acosta1, Hipatia Meza Intriago1, Aline Siteneski3*
1 Academic Master's Degree with a Professional Trajectory in Early Childhood Education, Postgraduate Faculty, Universidad Técnica de Manabí, Portoviejo, Manabí, Ecuador
2 Department of Mathematics and Statistics, Faculty of Basic Sciences, Universidad Técnica de Manabí, Portoviejo, Ecuador. [email protected]
3* Research Institute, Faculty of Health Science, Medicine Career and Department of Social and Behavioral Sciences, Psychology Degree, Manabí, Ecuador. *[email protected]
Correspondence: [email protected]
Available from: http://dx.doi.org/10.21931/RB/2023.08.03.93
ABSTRACT
The Anxiety Disorder diagnosis is a common comorbidity of Children with Autism Spectrum Disorder (ASD). The early detection of Anxiety is essential to increase the quality of life of children, especially in kindergarten children. Thus, the study aimed to investigate the differences between parents and teachers in reports of Anxiety in autistic children 3–5 years old. We used the Screen for Child Anxiety-Related Disorders (SCARED) parent version for parents and teachers of Ecuadorian children with ASD. The statistical analyses were performed on two evaluations of the same children. The sample size was 34 parents and 34 teachers. The binomial logistic regression model for the SCARED rating to the responses of teachers was statistically significant for age (odds [OR], 0.16; 95% confidence interval [CI] 0.31-0.82) for 5-year-olds (p<0.028). The SCARED subscale for Panic Disorder, Generalized Anxiety Disorder, Separation Anxiety Disorder, and Social Anxiety Disorder is correlated with the anxiety disorder. The data are statistically significant based on teachers' responses (p <0.05). According to parents' responses, the SCARED rating did not find any relationship between the study variables and the anxiety disorder. Most children were classified with anxiety disorder when evaluated by teachers but not by parents. Identifying Anxiety in children with ASD in kindergarten can help adequately treat the disease and contribute to neurodevelopment and quality of life in childhood.
Keywords: Anxiety Disorder; Children; Autism; Kindergarten; Ecuador
INTRODUCTION
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder with heterogeneous characteristics that depend on genetic and environmental factors 1,2. Difficulties in social communication and restricted and repetitive behaviors are observed in children with ASD 3. Recent studies focus their efforts on the early diagnosis of autism 4,5. However, although risk factors are considered, the diagnosis of autism is still based on specialized medical expertise with diagnostic instrumentation 6. Individuals with ASD are likelier to develop comorbidity such as psychiatric disorders 7,8. Young people with ASD have higher levels of Anxiety when compared to children with typical development 8.
Anxiety disorders are among children's most common neuropsychiatric disorders and can be diagnosed in kindergarten 9,10,11. However, information on the prevalence of anxiety disorders during early childhood is relatively scarce 12,13. Prevalence rates of Anxiety among kindergarten children range in different countries from 2 to 20% 9,10,11. Unfortunately, in children with ASD, the estimated prevalence rate is 40% 8.
Anxiety disorder is a negative, vague, and unpleasant emotional state derived from anticipating potential danger. Anxiety leads to the potentiation of alertness and hypervigilance behavior even without immediate danger 14. According to the Diagnostic and Statistical Manual of Mental Illnesses 3, Anxiety can be categorized into generalized anxiety disorder, panic disorder, agoraphobia, phobias, and social anxiety disorder 15. Anxiety during childhood, adolescence, or adulthood increases the risk of developing depressive disorders with more severe symptoms, such as resistant depressive disorders or suicide attempts 16,17. Early identification of anxiety disorders in children is of substantial public health importance. The Screen for Child Anxiety and Related Emotional Disorders (SCARED) is a widely used questionnaire to detect early Anxiety in children 18 and children with ASD 19.
Integrating multiple responses, such as parent and child anxiety scales, may lead to a more assertive diagnosis of Anxiety in children 20,21. However, the meaning of the different scores on the anxiety scales and how to integrate the discrepant results to generate a conclusion represent a challenge for researchers and clinicians. Several studies attempted to relate the differences between the responses of children and their parents to anxiety symptoms 22,21,23. Parents commonly report fewer symptoms than their children on anxiety scales 23,24,25. In kindergarten children, the alternative is to use a diagnostic anxiety scale answered by the parents 21. To our knowledge, no data compares the responses of parents and teachers of kindergarten children with ASD. Early diagnosis of Anxiety in autistic children allows adequate and tailored intervention. Accurate diagnosis of anxiety disorder depends on multiple evaluations, especially in autistic children. Thus, our research aimed to evaluate Anxiety in kindergarten children and compared the responses of parents and teachers of children with ASD.
MATERIALS AND METHODS
Study design
We performed a prospective cross-sectional study in Ecuador, including a sample of teachers and parents of autism spectrum disorder (ASD) children clinically diagnosed with Childhood Autism 26. Data collection occurred between September 2022 and December 2022. The manuscript was written with STROBE recommendations 27.
Setting
The study was performed in (Portoviejo, Manta and El Carmen), a coastal region in Ecuador (South America).
Eligibility Criteria and Outcomes
Teachers and parents of children with autism spectrum disorder (ASD) participated in the study. The inclusion criteria for samples were children between 3 and 5 years old. Teachers and parents of children with ASD previously diagnosed by each child's clinician were invited to participate. Only complete questionnaires were included. The final analyses were performed with completed questionnaires of the children themselves, both in the responses of parents and teachers. General Anxiety Disorder was considered the primary outcome. The range of questions and scores for Panic Disorder or Significant Somatic Symptoms, Generalized Anxiety Disorder, Separation Anxiety Disorder, Social Anxiety Disorder, and School Avoidance were considered secondary outcomes.
Data sources/measurement
The analyses included two evaluations of the same children. The statistical analyses were performed with children to whom two online questionnaires were applied (parents and teachers). The sample size was 34 parents and 34 teachers of ASD children.
Anxiety symptoms of ASD children
Parents and teachers of ASD children should indicate how often they have observed each symptom over the last 3 months. The Screen for Child Anxiety Related Disorders (SCARED) parent version assessed anxiety symptoms in kindergarten children. The SCARED is a 41-item questionnaire developed to assess different characteristics of Anxiety in children and ASD children 18,19. It is available in self-report and parent-report formats. This questionnaire of forty-one items measures Anxiety in children: "0 for no and 2 for true". Ranges from a total score of ≥ 25 may indicate the presence of an Anxiety Disorder. Scores above 30 are more specific for anxiety disorder. Each question may correlate with scores following: Significant School Avoidance may be represented by a score of 3 on items 2, 11, 17, and 36. A score of 5 on items 4, 8, 13, 16, 20, 25, 29, and 31 may indicate Separation Anxiety Disorder. A score of 7 for the items in questions 1, 6, 9, 12, 15, 18, 19, 22, 24, 27, 30, 34, and 38 may indicate Panic Disorder or Significant Somatic Symptoms. Social Anxiety Disorder may be represented by a score of 8 on items 3, 10, 26, 32, 39, 40, and 41. Finally, the high score of 9 on questions 5, 7, 14, 21, 23, 28, 33, 35, and 37 may indicate Generalized Anxiety Disorder. The psychometric properties of the SCARED were previously tested 28 with (= 0.90) internal consistency for the parent-report version for the overall score and ranged from satisfactory (= 0.73 for school avoidance) to good (= 0.89 for social phobia) for the subscales. The measure's sensitivity for diagnosing anxiety disorders in autistic youth was 0.71, and its specificity was 0.67 28.
Sociodemographic information of students
The sociodemographic variables, age, sex, race and place of residence, were recorded, in addition to data from the information about the parents' responses to the questionnaire.
Statistical Analysis
The descriptive statistical analysis was based on continuous, categorical, or ordinal variables presented in frequencies (N) and percentages (%) to describe the sociodemographic characteristics of children. Shapiro-Wilk test was used, and univariate analyses were performed using the Chi-square test. A logistic regression was conducted to find factors predicting the presence and absence of Anxiety. Binary logistic regression was used to determine whether or not a correlation existed between the responses given by parents and teachers. The SCARED scale evaluates the anxiety disorder in a child with autism. The variables considered in the model were age, sex, place of residence (zone), school year, and disorders according to the scale mentioned above. The adjusted odds ratio (OR), 95% confidence interval (95% CI), and p-value were used to express the possible correlations. Box plots were also produced to determine general trends according to the significant variables (p < 0.05). The significance level was set at α=0.05, and the statistical analyses were performed in SPSS 26 (IBM).
RESULTS
A total of 34 parents and 34 teachers of children completed the questionnaires. This study assessed the differences between the responses of parents and teachers of autistic children with autism spectrum disorder (ASD) on the Ecuadorian coast. The Screen for Child Anxiety-Related Disorders (SCARED) was available. The complete SCARED of teachers and parents was included in the statistical analysis (Fig 1).
Descriptive data
Table 1 shows the results of different sociodemographic characteristics.
Sociodemographic characteristics
A total of 34 participants between 3 to 5 years old (mean age = 4.41 years), 8 girls (23.53%) and 26 boys (76.47%), were included in the study, and 94.12% of the study population is located in the urban area, and 73.53% is of mixed race.
Anxiety disorder in kindergarten children with ASD
Table 2 shows that the scores according to the SCARED rating for teachers and parents do not have significant differences, which means they agree on the responses based on the child's behavior. However, it can be highlighted that more than 50% of the participants in this study have emotional disorders.
Anxiety disorder for parents and teachers of kindergarten children with ASD
The results of binary logistic regression analysis predict optimistic results for anxiety disorders in kindergarten children. The SCARED scale was responses from parents and teachers of kindergarten children. The binomial logistic regression model for the SCARED rating according to the responses of teachers was statistically significant for age (odds [OR], 0.16; 95% confidence interval [CI] 0.31-0.82) for 5-year-olds (p<0.028). This result shows a positive correlation between higher child age and higher Anxiety. Our results found differences in the school year (odds [OR], 6.22; 95% confidence interval [CI] 1.212-31.937) referring to initial sublevel 1 (p <0.029). These results represent the different types of Anxiety concerning each school year evaluated.
On the other hand, School Avoidance was not correlated with the anxiety disorder of children with ASD. It should be noted that the SCARED subscale for Panic Disorder, Generalized Anxiety Disorder, Separation Anxiety Disorder, and Social Anxiety Disorder are correlated with anxiety disorder, and the data are statistically significant based on the responses of teachers (p <0.05) (Table 3). Curiously, according to the parent's responses, the binomial logistic regression for the SCARED rating did not find any relationship between the study variables and the anxiety disorder (Table 3).
According to the binomial logistic regression analysis, there are statistically significant differences for Anxiety evaluated by teachers with the SCARED scale (p <0.05). The diagrams in each box represent significant values (***) for panic disorder, generalized anxiety disorder, separation anxiety disorder, and social anxiety disorder when directly correlated with anxiety disorder. However, according to parents' responses, there is no correlation between the SCARED subscales.
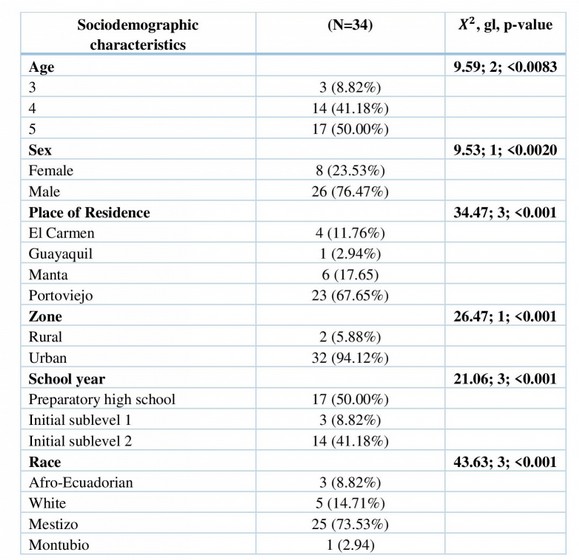
Frequency (percentage), Note: χ2 = check chi-square; gl = degrees of freedom; p = statistical significance.
Table 1. Sociodemographic data of kindergarten autism children
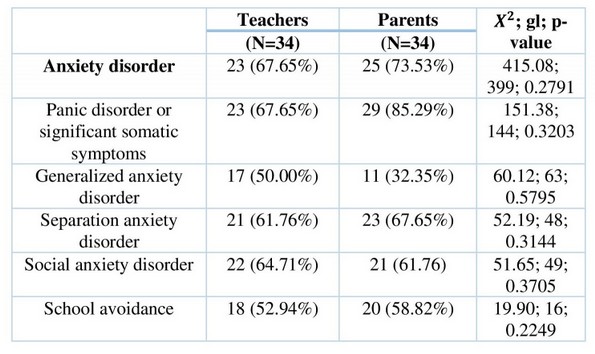
Frequency (percentage), Note: χ2 = check chi-square; gl = degrees of freedom; p = statistical significance.
Table 2. SCARED responses from parents and teachers of kindergarten children
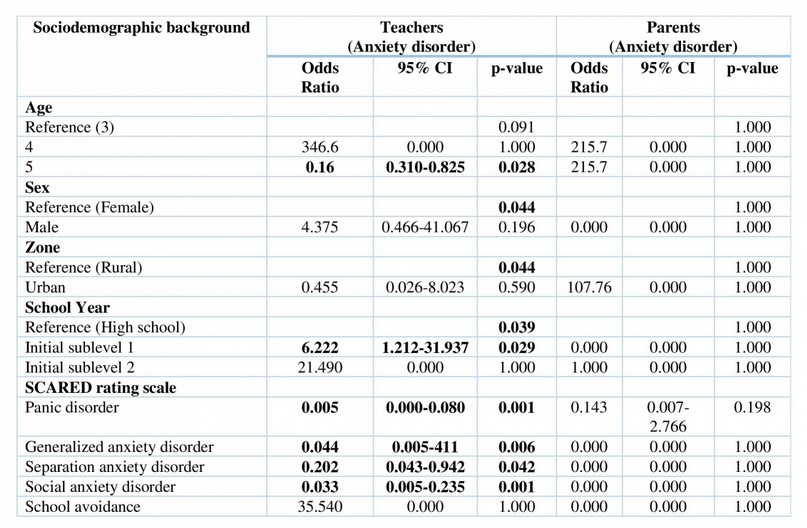
Note: OR = odds ratio; 95% CIs = 95% Confidence Intervals; Statistically significant effects (p < .05) are in bold. Panic disorder or Significant Somatic symptoms PD; Generalized Anxiety disorder= GAD; Separation Anxiety Disorder= SAD; Social anxiety disorder = SF; School Avoidance= SA; Anxiety disorder = AD.
Table 3. Binary logistic regression analysis for anxiety disorder using SCARED and sociodemographic data from responses of teachers and parents of kindergarten children with ASD.
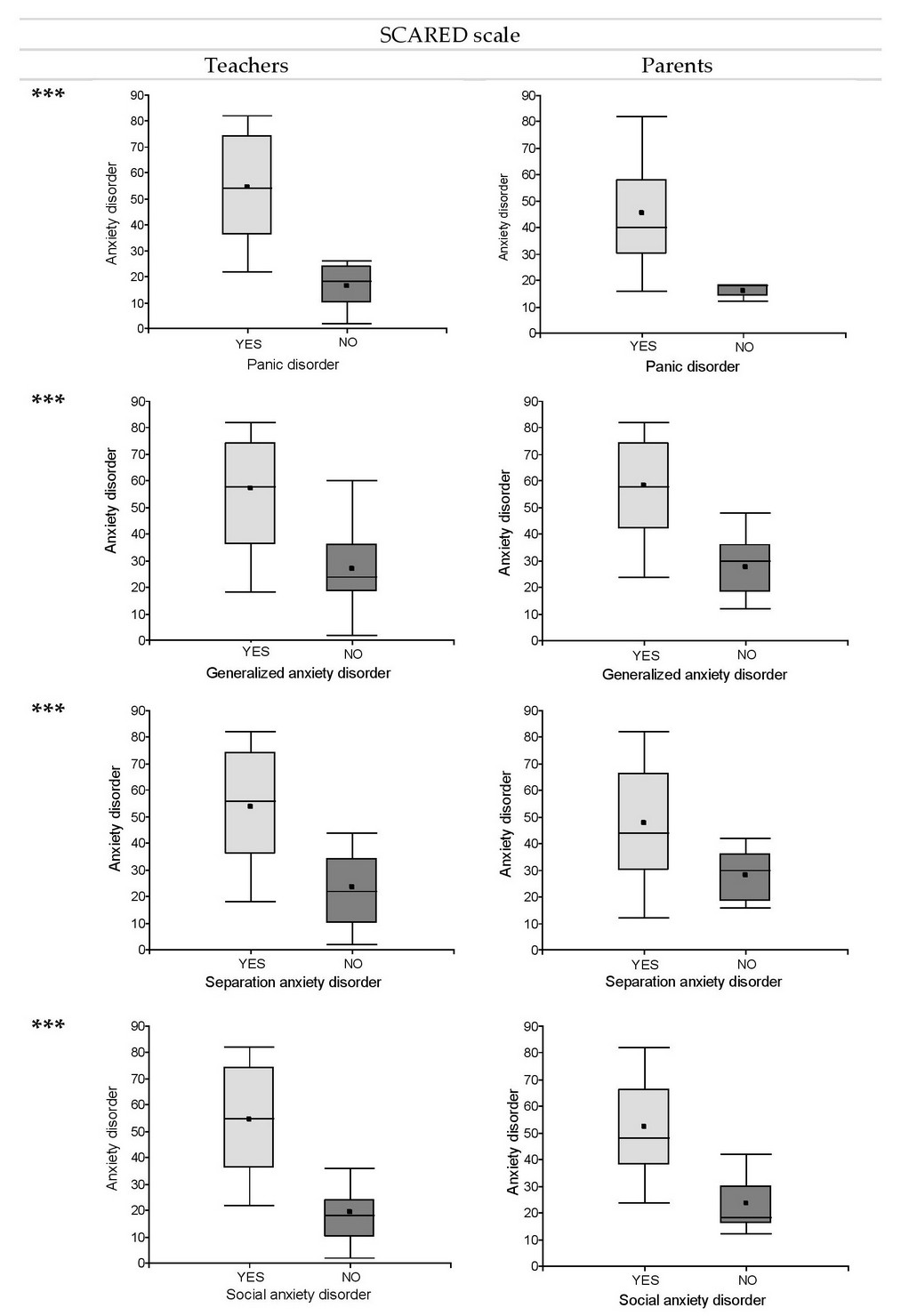
Figure 1. Boxplot to compare parent responses according to the SCARED scale. The red line represents the scores to determine each disorder: Generalized Anxiety Disorder (score of 9), Social Anxiety Disorder (score of 8), and School Avoidance (score of 3).
DISCUSSION
This study aimed to provide information about anxiety disorder in kindergarten children with ASD. We compared the SCARED responses from parents and teachers of children with ASD. Our results showed that anxiety disorder levels increase in older kindergarten children compared to younger ones (3 to 5 years old, respectively). In the scoring, SCARED Panic disorder or Significant Somatic Symptoms, generalized anxiety disorder, Separation Anxiety Disorder, Social anxiety disorder, and Anxiety disorder were significant for teachers' responses about kindergarten children with ASD. Interestingly, none of the SCARED scores subscales for Anxiety were positive for parents of the same kindergarten children with ASD evaluated.
Anxiety disorders in children and adolescents are associated with high morbidity rates and psychiatric disorders in adult life 29,30. Anxiety is among the most common disorders in people with ASD 31. Approximately 40% of children with ASD are diagnosed with at least one comorbid anxiety disorder, such as generalized anxiety disorder or social anxiety 32. One hypothesis that explains children with ASD have a neurobiological predisposition to cause ASD-related difficulties. The neurobiological factors, in combination with environmental factors such as bullying and parenting, may increase the potential anxiety disorder 32. In particular, Anxiety in ASD younger people is associated with further social impairment, self-injurious behavior, depressive symptoms, gastrointestinal problems, and increased stress in parents with ASD 33,34,35. Already in adults, the diagnosis of ASD is correlated with an increased risk of Anxiety and depressive disorder 36.
In our study, the older kindergarten children obtained higher scores on Anxiety than younger children with ASD in the teacher's evaluation. Early diagnosis and treatment of Anxiety in children with ASD are essential to children's social interaction in the school environment. Difficulties in social cognition in children and adolescents with ASD can increase Anxiety in social situations 37,21,38. In addition, Anxiety coupled with poor social skills can worsen interactions with peers, reducing the child's quality of life 39,32.
Children with ASD exhibit abnormal behaviors, including impairments in social interaction, communication, and repetitive behavior patterns 40,41. We found increased social Anxiety in the responses of teachers of children with ASD in kindergarten. Previous studies report that children with ASD usually have few friends and are disconnected from the social environment at school 42,43. Children and adolescents with ASD commonly experience social and academic challenges within the school environment in addition to possible cognitive, motor, and language deficits 44. Increased social Anxiety in children with ASD in kindergarten can hinder the ability to interact in the school environment. In fact, in patients with ASD, social anxiety disorder causes qualitative impairments in communication and social interaction in the early stages of life 3.
Children with ASD have high levels of social anxiety disorder 39,45. Children with ASD have sensory hypersensitivity, difficulties taking perspective, and limited socializing ability. 3. Social isolation and quietness in social situations are characteristic features of social anxiety disorder and expected behaviors in ASD children 46. Another hypothesis is that the experience of repeated rejection in a child with ASD 47,48 could result in social Anxiety and avoidance 49. In our study, kindergarten children have high social anxiety scores when evaluated by teachers.
The SCARED allows the assessment of Panic disorder or Significant Somatic Symptoms. Panic disorder represents physiological and cognitive symptoms for the patient. The anticipatory Anxiety and phobic avoidance clusters associated with recurrent and unexpected panic attacks are some of the symptoms experienced by the patient 3,50. Previous studies report that the structure of the amygdala in the brain is related to the pathophysiology of panic disorder 51,52. Anxiety disorder in children with ASD is associated with alterations in the structure of the amygdala in the brain 53. Regarding the work on the Rating Scale about Panic Disorder or Significant Somatic Symptoms in kindergarten children, we showed high levels in teachers' evaluation and no positive scores in parents' evaluation.
The SCARED scale applied to parents and children appears trustworthy 54. SCARED is commonly used to quantify anxiety symptoms during childhood and adolescence 55,56. The SCARED generally shows moderate correlations between child- and parent-reported scores, especially for the social Anxiety subscale 25,18,57,58,20. Parents may report observable behaviors such as ritual, restlessness, insomnia, and discomfort in social situations as anxiety 59. We assessed the responses of parents and teachers and found disagreement in the scores for SCARED.
Teachers' reports of the clinical picture of generalized Anxiety can make the diagnosis reliable and valid 60. Teachers and parents perceive externalizing symptoms of ADHD similarly when asked to rate children with ASD, but they agree less when rating internalizing symptoms such as anxiety 61,62. In our study, the SCARED scores on four of the five sub-items evaluated were higher when teachers evaluated the children than when parents did. When it comes to general psychiatric symptoms, a previous study showed that teachers tend to report rates in students with ASD 63.
Strengths and limitations
This study has several limitations. Firstly, the sample must be more significant (increase sample) to generalize the results and may underestimate the effect of statistical data. Secondly, the scale applied does not allow for confirming the diagnosis of Anxiety. In addition, the type of study, an observational cross-sectional, does not provide information about the influence of anxiety levels in kindergarten over time. Other studies must be performed to enlarge the sample and monitor the anxiety levels of students with ASD in kindergarten and contribute to the neurodevelopment of these children.
On the other hand, the homogeneity of our sample provides an excellent external value. The kindergarten children aged between 3 to 5 years have been assessed. It should be noted that we found significant differences when we compared teachers' responses to children's Anxiety and no difference when the responses were from the children's parents. We evaluate responses from parents and teachers of the same children about Anxiety Disorder, which may contribute to the correct diagnosis. Additionally, we used the SCARED Rating Scale previously reported in ASD children to explore the quality of life, neurobiological underpinnings, and treatment 64,65,66,19. The anxiety disorder in autistic children may affect their neurodevelopment, social participation, and educational outcomes. Despite the impact of anxiety disorders on autistic children, few studies report on Anxiety in preschool children 8, 19. We also include two different assessments of the children. This study provides parents' and teachers' responses to anxiety disorder in autistic children. Few studies compare responses of parents and teachers about Anxiety in preschool children 20, 24, 35. Our findings highlight the importance of using comprehensive assessments to help diagnose Anxiety in autistic children. Although a small sample, the study contributes to the literature with data from the Ecuadorian population of children with autism. In addition, we provided a double assessment of the same child, highlighting the importance of assessing the teacher's opinion of the student's anxiety level.
CONCLUSIONS
In conclusion, these findings support the notion that early diagnosis of anxiety disorder is essential for kindergarten children with ASD. This is the first study about Anxiety in autistic children aged 3-5 years in Ecuador. In addition, we reinforce the importance of parents and teachers having a rating scale for children's anxiety symptoms. The discrepancy between the responses of teachers and parents may be responsible for underdiagnoses of Anxiety Disorder with severe consequences in the neurodevelopment of children with ASD.
Supplementary Materials: Not applicable.
Author Contributions: Conceptualization, Siteneski A; methodology, Siteneski A; formal analysis, Montes Escobar K; investigation, Loor Robles. VA; data curation, Montes Escobar K; writing—original draft preparation, Siteneski A. and Loor Robles. VA; writing—review and editing, Siteneski A and Montes Escobar K.; visualization, Zambrano Acosta JZ and Meza Intriago H.; supervision, Zambrano Acosta JZ.; funding acquisition, Zambrano Acosta JZ and Meza Intriago H.
Funding: Universidad Técnica de Manabí.
Institutional Review Board Statement: Not applicable.
Informed Consent Statement: In our study, each child was assigned a number. The teacher and parents of the participants in the survey provided written informed consent. The University Technical of Manabí's ethical committee of CEISH-UTM-INT-ART_23-4-26_VALR approved this study.
Data Availability Statement: Not applicable.
Acknowledgments: This study was supported by the Research Institute and Postgraduate Faculty, Universidad Técnica de Manabí, Portoviejo, Manabí, Ecuador.
Conflicts of Interest: The authors declare no conflict of interest.
REFERENCES
1. Hallmayer J, Cleveland S, Torres A, Phillips J, Cohen B, Torigoe T, et al. Genetic heritability and shared environmental factors among twin pairs with autism. Arch Gen Psychiatry. 2011;68(11):1095-102.
2. Sandin S, Lichtenstein P, Kuja-Halkola R, Larsson H, Hultman CM, Reichenberg A. The familial risk of autism. JAMA. 7 de mayo de 2014;311(17):1770-7.
3. American Psychiatric Association, American Psychiatric Association, editors. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Washington, DC: American Psychiatric Association; 2013. 947 p.
4. Lord C, Brugha TS, Charman T, Cusack J, Dumas G, Frazier T, et al. Autism spectrum disorder. Nat Rev Dis Primer. 16 de enero de 2020;6(1):5.
5. Wolff JJ, Gu H, Gerig G, Elison JT, Styner M, Gouttard S, et al. Differences in white matter fiber tract development present from 6 to 24 months in infants with autism. Am J Psychiatry. junio de 2012;169(6):589-600.
6. Millar L, McConnachie A, Minnis H, Wilson P, Thompson L, Anzulewicz A, et al. Phase 3 diagnostic evaluation of a smart tablet serious game to identify autism in 760 children 3-5 years old in Sweden and the United Kingdom. BMJ Open. 16 de julio de 2019;9(7):e026226.
7. Postorino V, Kerns CM, Vivanti G, Bradshaw J, Siracusano M, Mazzone L. Anxiety Disorders and Obsessive-Compulsive Disorder in Individuals with Autism Spectrum Disorder. Curr Psychiatry Rep. 30 de octubre de 2017;19(12):92.
8. van Steensel FJA, Heeman EJ. Anxiety Levels in Children with Autism Spectrum Disorder: A Meta-Analysis. J Child Fam Stud. 2017;26(7):1753-67.
9. Paulus FW, Backes A, Sander CS, Weber M, von Gontard A. Anxiety disorders and behavioral inhibition in preschool children: a population-based study. Child Psychiatry Hum Dev. febrero de 2015;46(1):150-7.
10. Franz L, Angold A, Copeland W, Costello EJ, Towe-Goodman N, Egger H. Preschool anxiety disorders in pediatric primary care: prevalence and comorbidity. J Am Acad Child Adolesc Psychiatry. diciembre de 2013;52(12):1294-1303.e1.
11. Steinsbekk S, Ranum B, Wichstrøm L. Prevalence and course of anxiety disorders and symptoms from preschool to adolescence: a 6-wave community study. J Child Psychol Psychiatry. mayo de 2022;63(5):527-34.
12. Costello EJ, Egger HL, Angold A. The developmental epidemiology of anxiety disorders: phenomenology, prevalence, and comorbidity. Child Adolesc Psychiatr Clin N Am. octubre de 2005;14(4):631-48, vii.
13. Egger HL, Angold A. Common emotional and behavioral disorders in preschool children: presentation, nosology, and epidemiology. J Child Psychol Psychiatry. 2006;47(3-4):313-37.
14. Davis M, Walker DL, Miles L, Grillon C. Phasic vs sustained fear in rats and humans: role of the extended amygdala in fear vs Anxiety. Neuropsychopharmacol Off Publ Am Coll Neuropsychopharmacol. enero de 2010;35(1):105-35.
15. DSM [Internet]. [2023]. Disponible en: https://www.psychiatry.org:443/psychiatrists/practice/dsm
16. Stein MB, Fuetsch M, Müller N, Höfler M, Lieb R, Wittchen HU. Social anxiety disorder and the risk of depression: a prospective community study of adolescents and young adults. Arch Gen Psychiatry. marzo de 2001;58(3):251-6.
17. Bilgiç A, Yilmaz S, Hergüner S. The impact of anxiety sensitivity on suicidality in adolescents with major depressive disorder. Psychiatr Danub. diciembre de 2017;29(4):473-9.
18. Birmaher B, Khetarpal S, Brent D, Cully M, Balach L, Kaufman J, et al. The Screen for Child Anxiety Related Emotional Disorders (SCARED): scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry. abril de 1997;36(4):545-53.
19. Schiltz HK, Magnus BE. Differential Item Functioning Based on Autism Features, IQ, and Age on the Screen for Child Anxiety Related Disorders (SCARED) Among Youth on the Autism Spectrum. Autism Res Off J Int Soc Autism Res. junio de 2021;14(6):1220-36.
20. Rappaport BI, Pagliaccio D, Pine DS, Klein DN, Jarcho JM. Discriminant validity, diagnostic utility, and parent-child agreement on the Screen for Child Anxiety Related Emotional Disorders (SCARED) in treatment- and non-treatment-seeking youth. J Anxiety Disord. octubre de 2017;51:22-31.
21. Jansen M, Bodden DHM, Muris P, van Doorn M, Granic I. Measuring Anxiety in Children: The Importance of Separate Mother and Father Reports. Child Youth Care Forum. 2017;46(5):643-59.
22. De Los Reyes A, Augenstein TM, Wang M, Thomas SA, Drabick DAG, Burgers DE, et al. The validity of the multi-informant approach to assessing child and adolescent mental health. Psychol Bull. julio de 2015;141(4):858-900.
23. Russell JD, Graham RA, Neill EL, Weems CF. Agreement in Youth-Parent Perceptions of Parenting Behaviors: A Case for Testing Measurement Invariance in Reporter Discrepancy Research. J Youth Adolesc. octubre de 2016;45(10):2094-107.
24. Weems CF, Taylor LK, Marks AB, Varela RE. Anxiety sensitivity in childhood and adolescence: Parent reports and factors that influence associations with child reports. Cogn Ther Res. 2010;34:303-15.
25. Behrens B, Swetlitz C, Pine DS, Pagliaccio D. The Screen for Child Anxiety Related Emotional Disorders (SCARED): Informant Discrepancy, Measurement Invariance, and Test-Retest Reliability. Child Psychiatry Hum Dev. junio de 2019;50(3):473-82.
26. Wing L, Gould J, Gillberg C. Autism spectrum disorders in the DSM-V: better or worse than the DSM-IV? Res Dev Disabil. 2011;32(2):768-73.
27. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 16 de octubre de 2007;4(10):e296.
28. Stern JA, Gadgil MS, Blakeley-Smith A, Reaven JA, Hepburn SL. Psychometric Properties of the SCARED in Youth with Autism Spectrum Disorder. Res Autism Spectr Disord. 1 de septiembre de 2014;8(9):1225-34.
29. Fineberg NA, Haddad PM, Carpenter L, Gannon B, Sharpe R, Young AH, et al. The size, burden and cost of disorders of the brain in the UK. J Psychopharmacol Oxf Engl. septiembre de 2013;27(9):761-70.
30. Mazzone L, Ruta L, Reale L. Psychiatric comorbidities in Asperger syndrome and high functioning autism: diagnostic challenges. Ann Gen Psychiatry. 25 de junio de 2012;11(1):16.
31. Yarger HA, Nordahl CW, Redcay E. Examining Associations Between Amygdala Volumes and Anxiety Symptoms in Autism Spectrum Disorder. Biol Psychiatry Cogn Neurosci Neuroimaging. septiembre de 2022;7(9):916-24.
32. van Steensel FJA, Bögels SM, Perrin S. Anxiety disorders in children and adolescents with autistic spectrum disorders: a meta-analysis. Clin Child Fam Psychol Rev. septiembre de 2011;14(3):302-17.
33. Kerns CM, Kendall PC, Zickgraf H, Franklin ME, Miller J, Herrington J. Not to be overshadowed or overlooked: functional impairments associated with comorbid anxiety disorders in youth with ASD. Behav Ther. enero de 2015;46(1):29-39.
34. Mazurek MO, Vasa RA, Kalb LG, Kanne SM, Rosenberg D, Keefer A, et al. Anxiety, Sensory Over-Responsivity, and Gastrointestinal Problems in Children with Autism Spectrum Disorders. J Abnorm Child Psychol. enero de 2013;41(1):165-76.
35. Sukhodolsky DG, Scahill L, Gadow KD, Arnold LE, Aman MG, McDougle CJ, et al. Parent-rated anxiety symptoms in children with pervasive developmental disorders: frequency and association with core autism symptoms and cognitive functioning. J Abnorm Child Psychol. enero de 2008;36(1):117-28.
36. Joshi G, Wozniak J, Petty C, Martelon MK, Fried R, Bolfek A, et al. Psychiatric comorbidity and functioning in a clinically referred population of adults with autism spectrum disorders: a comparative study. J Autism Dev Disord. junio de 2013;43(6):1314-25.
37. Cooper M, Martin J, Langley K, Hamshere M, Thapar A. Autistic traits in children with ADHD index clinical and cognitive problems. Eur Child Adolesc Psychiatry. 2014;23(1):23-34.
38. Pepper KL, Demetriou EA, Park SH, Song YC, Hickie IB, Cacciotti-Saija C, et al. Autism, early psychosis, and social anxiety disorder: understanding the role of social cognition and its relationship to disability in young adults with disorders characterized by social impairments. Transl Psychiatry. 26 de octubre de 2018;8:233.
39. Bellini S. Social Skill Deficits and Anxiety in High-Functioning Adolescents with Autism Spectrum Disorders. Focus Autism Dev Disabil. 2004;19:78-86.
40. Geschwind DH. Advances in autism. Annu Rev Med. 2009;60:367-80.
41. Molecular Autism [Internet]. BioMed Central. [citado 20 de marzo de 2023]. Disponible en: https://molecularautism.biomedcentral.com/
42. Bauminger N, Solomon M, Rogers SJ. Predicting friendship quality in autism spectrum disorders and typical development. J Autism Dev Disord. junio de 2010;40(6):751-61.
43. Kasari C, Locke J, Gulsrud A, Rotheram-Fuller E. Social networks and friendships at school: comparing children with and without ASD. J Autism Dev Disord. mayo de 2011;41(5):533-44.
44. May T, Rinehart N, Wilding J, Cornish K. The role of attention in the academic attainment of children with autism spectrum disorder. J Autism Dev Disord. septiembre de 2013;43(9):2147-58.
45. Kuusikko S, Pollock-Wurman R, Jussila K, Carter AS, Mattila ML, Ebeling H, et al. Social Anxiety in high-functioning children and adolescents with Autism and Asperger syndrome. J Autism Dev Disord. octubre de 2008;38(9):1697-709.
46. Eriksson JM, Andersen LM, Bejerot S. RAADS-14 Screen: validity of a screening tool for autism spectrum disorder in an adult psychiatric population. Mol Autism. 9 de diciembre de 2013;4(1):49.
47. Cappadocia MC, Weiss JA, Pepler D. Bullying experiences among children and youth with autism spectrum disorders. J Autism Dev Disord. febrero de 2012;42(2):266-77.
48. Bejerot S, Humble MB. Childhood clumsiness and peer victimization: a case–control study of psychiatric patients. BMC Psychiatry. 25 de febrero de 2013;13(1):68.
49. Bejerot S, Eriksson JM, Mörtberg E. Social anxiety in adult autism spectrum disorder. Psychiatry Res. 15 de diciembre de 2014;220(1-2):705-7.
50. Craske MG, Kircanski K, Epstein A, Wittchen HU, Pine DS, Lewis-Fernández R, et al. Panic disorder: a review of DSM-IV panic disorder and proposals for DSM-V. Depress Anxiety. febrero de 2010;27(2):93-112.
51. Kim JE, Dager SR, Lyoo IK. The role of the amygdala in the pathophysiology of panic disorder: evidence from neuroimaging studies. Biol Mood Anxiety Disord. 20 de noviembre de 2012;2:20.
52. Dresler T, Guhn A, Tupak SV, Ehlis AC, Herrmann MJ, Fallgatter AJ, et al. Revise the revised? New dimensions of the neuroanatomical hypothesis of panic disorder. J Neural Transm Vienna Austria 1996. enero de 2013;120(1):3-29.
53. Hennessy A, Seguin D, Correa S, Wang J, Martinez-Trujillo JC, Nicolson R, et al. Anxiety in children and youth with autism spectrum disorder and the association with amygdala subnuclei structure. Autism Int J Res Pract. 22 de octubre de 2022;13623613221127512.
54. Wigham S, McConachie H. Systematic Review of the Properties of Tools Used to Measure Outcomes in Anxiety Intervention Studies for Children with Autism Spectrum Disorders. PLoS ONE. 21 de enero de 2014;9(1):e85268.
55. Bowers ME, Reider LB, Morales S, Buzzell GA, Miller N, Troller-Renfree SV, et al. Differences in parent and child report on the Screen for Child Anxiety-Related Emotional Disorders (SCARED): Implications for investigations of social Anxiety in adolescents. J Abnorm Child Psychol. 2020;48:561-71.
56. Arab A, El Keshky M, Hadwin JA. Psychometric Properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED) in a Non-Clinical Sample of Children and Adolescents in Saudi Arabia. Child Psychiatry Hum Dev. agosto de 2016;47(4):554-62.
57. Cosi S, Canals J, Hernández-Martinez C, Vigil-Colet A. Parent-child agreement in SCARED and its relationship to anxiety symptoms. J Anxiety Disord. enero de 2010;24(1):129-33.
58. Dirks MA, Weersing VR, Warnick E, Gonzalez A, Alton M, Dauser C, et al. Parent and youth report of youth anxiety: evidence for measurement invariance. J Child Psychol Psychiatry. marzo de 2014;55(3):284-91.
59. Lohr WD, Daniels K, Wiemken T, Williams PG, Kelley RR, Kuravackel G, et al. The screen for child anxiety-related emotional disorders is sensitive but not specific in identifying Anxiety in children with high-functioning autism spectrum disorder: A pilot comparison to the Achenbach system of empirically based assessment scales. Front Psychiatry. 2017;8.
60. Kendall PC, Puliafico AC, Barmish AJ, Choudhury MS, Henin A, Treadwell KS. Assessing Anxiety with the Child Behavior Checklist and the Teacher Report Form. J Anxiety Disord. 2007;21(8):1004-15.
61. Pearson DA, Aman MG, Arnold LE, Lane DM, Loveland KA, Santos CW, et al. High concordance of parent and teacher attention-deficit/hyperactivity disorder ratings in medicated and unmedicated children with autism spectrum disorders. J Child Adolesc Psychopharmacol. 2012;22:284-91.
62. Kaat AJ, Gadow KD, Lecavalier L. Psychiatric symptom impairment in children with autism spectrum disorders. J Abnorm Child Psychol. agosto de 2013;41(6):959-69.
63. Kanne SM, Abbacchi AM, Constantino JN. Multi-informant ratings of psychiatric symptom severity in children with autism spectrum disorders: the importance of environmental context. J Autism Dev Disord. junio de 2009;39(6):856-64.
64. Reaven J, Blakeley-Smith A, Leuthe E, Moody E, Hepburn S. Facing your fears in adolescence: cognitive-behavioral therapy for high-functioning autism spectrum disorders and Anxiety. Autism Res Treat. 2012;2012:423905.
65. Herrington JD, Miller JS, Pandey J, Schultz RT. Anxiety and social deficits have distinct relationships with amygdala function in autism spectrum disorder. Soc Cogn Affect Neurosci. junio de 2016;11(6):907-14.
66. Smith IC, Ollendick TH, White SW. Anxiety moderates the influence of ASD severity on quality of life in adults with ASD. Res Autism Spectr Disord. 1 de junio de 2019;62:39-47.
Received: 25 June 2023/ Accepted: 26 August 2023 / Published:15 September 2023
Citation: Loor Robles V A, Montes-Escobar K, Zambrano Acosta J M, Meza In-triago H, Siteneski A. Differences between the responses of parents and teachers Anxiety screening for autistic children aged 3-5 years: a cross-sectional study. Revis Bionatura 2023;8 (3) 93 http://dx.doi.org/10.21931/RB/2023.08.03.93