2023.08.03.92
Files > Volume 8 > Vol 8 No 3 2023
Anxiety levels and school performance of Ecuadorian children from 3 to 5 years old: a cross-sectional study

Mayra Azucena Roldán Bazurto1 , Karime Montes-Escobar2, Jimmy Manuel Zambrano Acosta1, Hipatia Meza Intriago1 , Aline Siteneski3*
, Karime Montes-Escobar2, Jimmy Manuel Zambrano Acosta1, Hipatia Meza Intriago1 , Aline Siteneski3*
1 Academic Master's Degree with a Professional Trajectory in Early Childhood Education, Postgraduate Faculty, Universidad Técnica de Manabí, Portoviejo, Manabí, Ecuador. [email protected], ; [email protected] ; [email protected]
2 Department of Mathematics and Statistics, Faculty of Basic Sciences, Universidad Técnica de Manabí, Portoviejo, Ecuador. [email protected]
3* Research Institute, Faculty of Health Science, Medicine Carrier and Department of Social and Behavioral Sciences, Psychology Degree, Manabí, Ecuador
Correspondence author: [email protected]
Available from: http://dx.doi.org/10.21931/RB/2023.08.03.92
ABSTRACT
Anxiety Disorder is common in kindergarten children. The high rates of anxiety disorder impact neurodevelopment and consequently may contribute to poor school performance. Thus, this study aimed to evaluate the influence of anxiety rates on the school performance of kindergarten children. It used the Screen for Child Anxiety Related Disorders (SCARED) parent version in parents of Ecuadorian children. The statistical analyses included one hundred fourteen responses from parents of kindergarten children. The binomial logistic regression model for the SCARED rating for parents' answers was statistically significant for Generalized Anxiety Disorder (odds [OR], 0.036; 95% confidence interval and p <0.001. A statistically substantial score (odds [OR], 0.037; 95% confidence interval and p <0.001, was presented in Social Anxiety Disorder. Finally, school refusal was evaluated (odds [OR], 0.038; 95% confidence interval [CI] 0.004-0.340) with a (p <0.003). A positive statistical correlation between social disorder and school avoidance correlated with anxiety disorder in kindergarten children.
In conclusion, our results showed that Anxiety Disorders are common in kindergarten children. We did not find a correlation between anxiety levels and the school performance of our children sample. There is a positive relationship between anxiety and school avoidance in Ecuadorian children.
Keywords: Anxiety Disorder; Kindergarten; Children; School performance Social disorder; School avoidance.
INTRODUCTION
Diagnosing and preventing anxiety disorders is essential for the adequate neuro-development of kindergarten children 1. Children's anxiety can manifest through behavioral changes, such as fidgeting, shaking, taking deep breaths, stopping talking or crying 2. Anxiety disorder can be defined as a negative, vague, and unpleasant emotional state. Anxiety is derived from anticipating a potential danger and increases alertness and hypervigilance behavior, even without immediate danger 3. Anxiety disorders include generalized anxiety, panic, agoraphobia, specific phobias, and social anxiety disorder4. In all subtypes, the somatic, cognitive, and behavioral manifestations of anxiety seem to affect the normal functioning of the individual 4.
Anxiety disorders include the most common psychiatric disorders in children and adolescents, affecting approximately 6.5% of children and adolescents5-6. The estimated prevalence of anxiety disorder in Western countries is 10-20% of children between 3 and 6 years of age 7. Anxiety disorder is among the most frequent psychiatric disorders in kindergarten children 7. Children and adolescents represent a significant source of morbidity and are associated with later adult psychopathology and higher costs than any other mental health disorder 6. However, despite the high prevalence and significant morbidity, anxiety disorders in childhood and adolescence can be challenging to diagnose. Anxiety disorder can be confused with regular worries, fears, and shyness of normal development 8.
It is common for a low rate of children with anxiety to receive appropriate treatment 9. Notably, children with anxious parents are up to five times more likely than children of non-anxious parents 10. Another factor that influences the development of anxiety disorder is behavioral inhibition. In children, behavioral inhibition is the tendency to react to new or unfamiliar situations with fear, withdrawal, and avoidance11,12. Kindergartners identified as inhibited are more likely to develop an anxiety disorder later in childhood and adolescence 11. Anxiety is also influenced by negative emotionality, a temperamental construct characterized by irritability, negative mood, difficulty calming down, and intense adverse emotional reactions 12.
Anxiety and depression symptoms in kindergarten tend to persist throughout development 13-14. Previous studies have shown that up to 14% of kindergarten children have clinical levels of anxiety and depression 15-16. High rates of anxiety in children result in impaired neurodevelopment and consequent poor academic performance 17–19. It should be noted that less social interaction can negatively influence the school performance of children of kindergarten age 20. Identifying the presence of anxiety disorder in kindergarten children helps predict maladjustment and later school failure. There is no data on anxiety in the population of Ecuadorian children. Thus, the present research aims to investigate the levels of anxiety reported by parents of children between 3 and 5 years of age. In addition, we intended to relate whether anxiety levels influence school performance in kindergarten children.
MATERIALS AND METHODS
Study design
The sample of kindergarten children was included in the study. Data collection occurred between September 2022 and December 2022. The data were assessed in the Unidad Educativa ¨Emilio Bowen Roggiero¨.
Setting
This research is a cross-sectional study performed in Manta, on the coast of Ecuador (South America). Ecuador is a country in South America that shares borders with Colombia to the north and Peru to the south/east and has the Pacific Ocean to the west. The government is divided into four geographical regions: the Coast, Highlands (also known as Sierra), Amazon, and the Galapagos Islands.
Eligibility criteria and outcomes
The present study was performed with kindergarten children. The samples used as included criteria were children between 3 and 5 years old. The parents of the children were invited to participate. The uncompleted questionnaires were excluded, and the final analyses were performed with completed questionnaires from the same children for various questions. Total anxiety score is considered a primary outcomes. It verifies rates for Panic Disorder or Significant Somatic Symptoms, Generalized Anxiety Disorder, Separation Anxiety Disorder, Social Anxiety Disorder, and School Avoidance as a secondary outcome.
Data sources/measurement
The sample size was a total of 114 parents of kindergarten children. Only completed online questionnaires were considered for statistical analyses.
Anxiety Symptoms of Kindergarten Children by SCARED Parent Version
Children's parents responded to the Screen for Child Anxiety Related Disorders (SCARED) parent version. Indication of the response on how often each symptom has been observed in the last 3 months. SCARED, a previously validated 41-item questionnaire, assessed anxiety symptoms in children 21-22. The SCARED is available in self-report and parent-report formats. It is a questionnaire of forty-one items that measure the anxiety in children: "0 for no and 2 for true". Ranges from a total score of ≥ 25 may indicate the presence of an Anxiety Disorder. Scores higher than 30 are more specific. A score of 9 in items 5, 7, 14, 21, 23, 28, 33, 35, 37 could suggest Generalized Anxiety Disorder, while a score of 7 in items 1, 6, 9, 12, 15, 18, 19, 22, 24, 27, 30, 34, 38 may indicate Panic Disorder or Significant Somatic Symptoms. Similarly, a score of 8 in items 3, 10, 26, 32, 39, 40, 41 might be indicative of Social Anxiety Disorder, and a score of 5 in items 4, 8, 13, 16, 20, 25, 29, 31 could point to Separation Anxiety Disorder. Lastly, a score of 3 on items 2, 11, 17, and 36 may suggest the presence of significant school avoidance. The SCARED has psychometric properties of specificity and internal consistency for the parent-report version of children previously tested 21–23. The parents were instructed to respond to their children. "For each statement, select the circle corresponding to the answer to the question that best describes your child's behavior in the last three months ."The parents responded to the 41 questions in the SCARED-parent questionnaire 21–23. Each parent was invited to participate, signed the informed consent, and later answered the questions. All questionnaires were anonymized. Parents and children received the personal number and were unnamed during all investigations. The ethical committee of Universidad Tecnica de Manabí number CEISH-UTM-INTART_23-4-25_MARB approved this work.
Sociodemographic information of kindergarten children
The sociodemographic variables, age, sex, place of residence, and school year were recorded. In addition, the data about the status of school performance "initiated, in progress or acquired" for the learning process of the school year. It should be noted that this is the assessment model used in Ecuador to evaluate kindergarten children.
Statistical Analysis
The sociodemographic data of the general study population were examined using descriptive statistics based on continuous, categorical, or ordinal variables expressed in frequencies (N) and percentages (%). Shapiro-Wilk and the Chi-square tests were used for univariate analyses. A binary logistic regression analysis was performed to identify positive predictors for the presence and absence of anxiety. The following variables were considered for the model: age, sex, place of residence, and the model of three evaluations of the learning process of the children's school year. The odds ratio (OR) was adjusted, and the 95% confidence interval (95% CI) was considered to express the possible correlations. Box plots were also produced to determine general trends according to the significant variables (p < 0.05). The significance level was set at α=0.05, and the statistical analyses were performed in SPSS 26 (IBM).
RESULTS
A total of 114 parents of kindergarten children completed the questionnaires. This study assessed the response of parents of children from rural and urban areas of the Ecuadorian coast. The Screen for Child Anxiety Related Disorders (SCARED) was evaluated. Only parents' completed SCARED were included in the statistical analyses (Fig 1). In the statistical analyses (Fig 1), only the complete SCARED of parents were included.
Descriptive data
Anxiety symptoms of kindergarten children
The results of the different sociodemographic characteristics are shown in Table 1. A total of 114 participants between 3 to 5 years old (mean age = 4.26 years), 53 girls (46.49%) and 61 boys (53.51%), were included in the study, and 95.61% of the study population was located in urban areas. It can also be observed that there are significant differences between the ages and the regions in which the participants are located for this study. We found differences between sex and school year among the participants.
Table 2 shows the scores according to the SCARED rating based on the parents' responses. Among the 114 participants, 11.40% had panic disorder, 29.82% separation anxiety disorder, avoidance school 5.26%, and 3.51% presented anxiety disorder symptoms. It is worth mentioning that no significant differences were found in children when we evaluated generalized anxiety disorder or social anxiety disorder according to the SCARED scale answered by parents. Finally, we assessed the stages of the learning process: "initiated, in progress, and acquired." No children were found in the initiated stage; 59.65% are in the progress stage, and 37.72% are in the acquired learning process.
Main results
Anxiety disorder for parents of kindergarten children
Binary logistic regression analysis values/assesses anxiety disorder scores with the SCARED scale responses of parents of kindergarten children (Table 3). The binomial logistic regression model for the SCARED rating according to the responses of the parents was statistically significant for Generalized Anxiety Disorder (odds [OR], 0.036; 95% confidence interval [CI] 0.000) with a (p <0.001). We observed in Social Anxiety Disorder a statistically significant score (odds [OR], 0.037; 95% confidence interval [CI] 0.000) with a (p <0.001). Finally, school avoidance was evaluated (odds [OR], 0.038; 95% confidence interval [CI] 0.004-0.340) with a (p <0.003). Our data demonstrate a positive statistical correlation between social disorder and school avoidance disorder correlated with anxiety disorder in kindergarten children.
There were no statistical differences when we compared the learning process stages and the Anxiety Disorder levels. We used box plots in Figure 1 to represent the statistically significant SCARED subscales in kindergarten children (*). According to the binomial logistic regression analysis, the general results of the study show meaningful differences between the parents' responses to the SCARED scale for school avoidance are statistically correlated (p <0.05) with anxiety disorder.
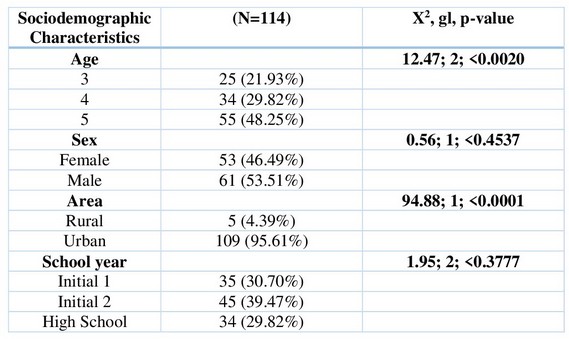
Frequency (percentage), Note: χ2 = check chi-square; gl = degrees of freedom; p = statistical significance.
Table 1. Sociodemographic data of kindergarten children.
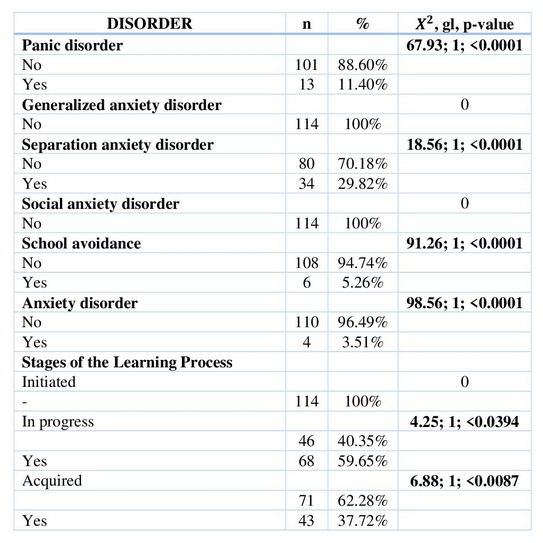
Frequency (percentage), Note: χ2 = check chi-square; gl = degrees of freedom; p = statistical significance.
Table 2. Data from the SCARED Rating Scale for Anxiety Disorder and school performance in kindergarten children.
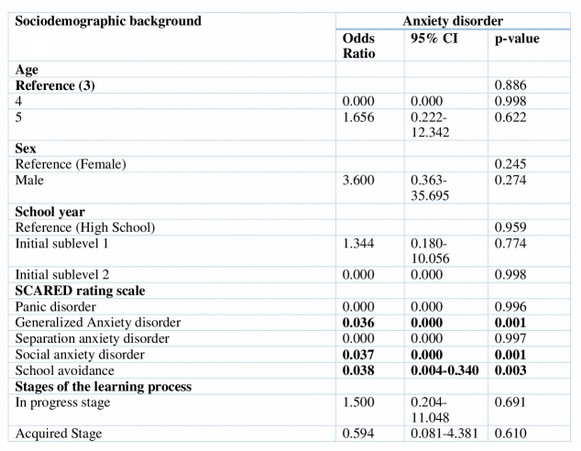
Note: OR = odds ratio; 95% CIs = 95% Confidence Intervals; Statistically significant effects (p < .05) are in bold. Panic disorder or Significant Somatic Symptoms= PD; Generalized anxiety disorder= GAD; Separation Anxiety Disorder= SAD; Social anxiety disorder = SAD; School Avoidance= SR; Anxiety disorder = AD.
Table 3. shows the binary logistic for anxiety using the parents' response to the SCARED about kindergarten children.
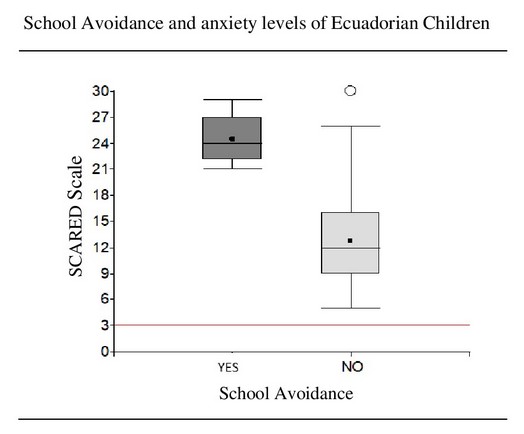
Figure 1. Figure 1. Boxplot to compare parent responses according to the SCARED scale. The red line represents the scores to determine School Avoidance (score of 3).
DISCUSSION
The present study reinforces and extends the notion that Anxiety Disorder in kindergarten children needs adequate diagnosis. Our results showed a positive correlation between Anxiety disorder and Generalized Anxiety Disorder, Social Anxiety Disorder, and School Avoidance. These results correspond to parents' SCARED response of 3-5-year-old children. The homogeneity of our sample suggests that Anxiety Disorders initiated in kindergarten should receive more attention. We did not find a correlation between anxiety levels and the school performance of kindergarten children. The sample size may influence the no correlation statistical significance.
Anxiety is the brain's response to danger, a stimulus that the body constantly tries to avoid 9. Anxiety disorders in kindergarten children are among the most common psychiatric disorders 7. The estimated prevalence of anxiety disorder in Western countries among children aged 3-5 years is 10-20% 5. We did not find differences between the anxiety scores and the age of the children. The small sample size probably influences the negative significance of our study; studies with a more significant number of students evaluated are necessary.
Anxiety is associated with short- and long-term impairment in social, academic, family, and psychological functioning 24. By not controlling daily events, children with anxiety disorder exhibit anguish and difficulty carrying out academic activities 25. Our results showed high rates of Social Anxiety Disorder. Kindergarten children generate anxiety during neurodevelopment for most phobias, separation anxiety, and other social anxiety disorders 1. It is common for children with anxiety disorder to worry more about school performance and family matters than children with other types of disorders 26. However, a previous study reported that kindergarten children with anxiety disorders did not have difficulty adapting to the school environment 27.
Anxiety disorders begin in childhood and adolescence, exhibit a homotypic continuity, and increase the risk of secondary anxiety and mood disorders 28. People with mental disorders have a lower life expectancy of 10 to 15 years than the general population 29. Anxiety disorders in adults have been associated with biased processing of emotional information that may be due to deficits in attentional control 30. Anxiety disorders in adults lead to hypervigilance and selective attention to threatening information. However, there is little information on attentional biases in anxious children 30. We found high levels of School Avoidance for the SCARED scale.
Although previous studies report high rates of Separation Anxiety Disorder in children 22-31-32, in our study in the hub, there are statistically significant differences for Separation Anxiety Disorder. Anxious children are less likely to interact spontaneously with an experimenter and more likely to show symptoms of generalized social anxiety in adolescence 33. Additionally, stable fear throughout childhood development has been considered a predictor of anxiety syndrome symptoms 34. Our study uses the SCARED scale to diagnose anxiety disorders in kindergarten children. The scale is widely used to assess anxiety symptoms and syndromes and has been evaluated in samples of preschoolers in cross-sectional and longitudinal surveys 21-28-35. The SCARED scale classifies symptoms of panic, separation anxiety, social phobia, generalized anxiety disorder, and school 21-36. In our study, none of the SCARED subscales is correlated with kindergarten children's school performance. It is essential to recognize childhood anxiety disorders to prevent normal psychosocial development in children. In addition, one of the main objectives of early diagnosis is to prevent future psychiatric disorders 37–39.
The prevalence of anxiety disorder plus depression in preschoolers is 13.4% worldwide 5. A meta-analysis of 41 studies evaluating 27 regions of the world detected an anxiety rate in children of 6.5% 5. In the United States, anxiety is the most common mental disorder in children and young people 40. In children, the psycho-therapeutic and pharmacological treatment for generalized, social, and separation anxiety disorders is feasible once diagnosed 28. However, treatment depends on a proper diagnosis. Despite the small sample size, our study seeks to contribute to the diagnosis of anxiety in kindergarten children. Despite high rates of anxiety and depressive symptoms in childhood, it is common not to identify the need for intervention 41. In Ecuador, there is no data on anxiety disorder in kindergarten children.
Mental disorders in childhood can adversely affect healthy development 42. Anxiety is the most common of these negative responses, and high levels of the condition can harm children's physiological and psychological health 43, 44. Childhood anxiety interferes with children's ability to achieve social, emotional, cognitive, and academic milestones and to function in daily environments 42. Furthermore, anxiety disorder in pediatric patients can impair self-confidence, social interactions, and cognitive ability 45. However, our study found no association between anxiety levels and school performance in kindergarten children. Unfortunately, children with anxiety disorders are more likely to develop mental health problems later in life 46.
Strengths and limitations
The researchers acknowledge that this study has multiple limitations. Firstly, due to the observational cross-sectional design of the study, there is no information about the long-term effects of anxiety levels in kindergarten. Secondly, the researchers must increase the sample size to generalize the results. The small sample of our study may need to be more accurate in the effect of statistical data. Furthermore, we used the SCARED scale in this study, which does not provide a conclusive diagnosis of anxiety.
On the other hand, the homogeneity of our sample adds external validity to the study, as it focuses specifically on kindergarten children between the ages of 3 and 5 years. Although there are several studies on anxiety in kindergarten children 5,7,26, we report data on Ecuadorian children. Children's social, emotional, and academic development is known to be affected by early anxiety disorder. Further studies are needed to extend the results of our research and provide data on the prevalence of Anxiety Disorder in Ecuadorian children. In underdeveloped countries, the impact of Anxiety Disorder in children can be significant. In the future, the generated data will draw attention to implementing public school policies to treat anxiety in children adequately.
CONCLUSIONS
In conclusion, our results showed that Anxiety Disorder is frequent in kindergarten children, and the disorder was independent of school performance. Cultural, social, and environmental factors may influence children's anxiety levels. To our knowledge, this is the first study to assess anxiety in kindergarten children in Ecuador. In particular, our results showed a positive association between anxiety levels and school avoidance among Ecuadorian children. Aspects such as socioeconomic factors, parenting styles, and educational systems may have contributed to our results and deserve more attention. Further studies are needed to increase the sample size and show the specific aspects correlated with the anxiety of Ecuadorian children.
Supplementary Materials: Not applicable.
Author Contributions: Conceptualization, Siteneski A; methodology, Siteneski A; formal analysis, Montes Escobar K; investigation, Roldán Bazurto MA.; data curation, Montes Escobar K; writing—original draft preparation, Siteneski A.; writing—review and editing, Siteneski A and Montes Escobar K.; visualization, Zambrano Acosta JZ and Meza Intriago H.; supervision, Zambrano Acosta JZ.
Funding: Universidad Técnica de Manabí.
Institutional Review Board Statement: Not applicable.
Informed Consent Statement: This study was approved by the Universidad Tecnica de Manabí's ethical committee CEISH-UTM-INTART_23-4-25_MARB.
Data Availability Statement: Not applicable.
Acknowledgments: This study was supported by the Research Institute and Postgraduate Faculty, Universidad Técnica de Manabí, Portoviejo, Manabí, Ecuador.
Conflicts of Interest: The authors declare no conflict of interest.
REFERENCES
1. Solmi M, Radua J, Olivola M, Croce E, Soardo L, Salazar de Pablo G, et al. Age at onset of mental disorders worldwide: a large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. 2022 Jan 2;27(1):281–95.
2. KainZeev N., Mayes Linda C. Anxiety in children during the perioperative period. In Child development and behavioral pediatrics. Morton N, editor. 2014. 85–104 p.
3. Davis M, Walker DL, Miles L, Grillon C. Phasic vs Sustained Fear in Rats and Humans: Role of the Extended Amygdala in Fear vs Anxiety. Neuropsychopharmacology. 2010 Jan 19;35(1):105–35.
4. Quinn Brian. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Primary Care Version. Prim Care Companion J Clin Psychiatry. 2013 Feb;1(2):54–5.
5. Polanczyk G V., Salum GA, Sugaya LS, Caye A, Rohde LA. Annual Research Review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry. 2015 Mar;56(3):345–65.
6. Fineberg NA, Haddad PM, Carpenter L, Gannon B, Sharpe R, Young AH, et al. The size, burden and cost of brain disorders in the UK. Journal of Psychopharmacology. 2013 Sep 24;27(9):761–70.
7. Whalen DJ, Sylvester CM, Luby JL. Depression and Anxiety in Preschoolers. Child AdolescPsychiatrClin N Am. 2017 Jul;26(3):503–22.
8. NICE (National Institute for Health and Care Excellence). Social Anxiety Disorder: Recognition, Assessment and Treatment. UK; 2013.
9. Pine DS, Helfinstein SM, Bar-Haim Y, Nelson E, Fox NA. Challenges in Developing Novel Treatments for Childhood Disorders: Lessons from Research on Anxiety. Neuropsychopharmacology. 2009 Jan 27;34(1):213–28.
10. Beidel DC, Turner SM. At Risk for Anxiety: I. Psychopathology in the Offspring of Anxious Parents. J Am Acad Child Ad-olesc Psychiatry. 1997 Jul;36(7):918–24.
11. Biederman J, Hirshfeld-Becker DR, Rosenbaum JF, Hérot C, Friedman D, Snidman N, et al. Further Evidence of Association Between Behavioral Inhibition and Social Anxiety in Children. American Journal of Psychiatry. 2001 Oct;158(10):1673–9.
12. GUZE SB. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV). American Journal of Psychiatry. 1995 Aug;152(8):1228–1228.
13. Briggs-Gowan Mj, Carter As, Bosson-Heenan J, Guyer Ae, Horwitz Sm. Are Infant-Toddler Social-Emotional and Behavioral Problems Transient? J Am Acad Child Adolesc Psychiatry. 2006 Jul;45(7):849–58.
14. Mesman J, Bongers IL, Koot HM. Preschool Developmental Pathways to Preadolescent Internalizing and Externalizing Problems. Journal of Child Psychology and Psychiatry. 2001 Jul 8;42(5):679–89.
15. Bayer JK, Hiscock H, Ukoumunne OC, Price A, Wake M. Early childhood etiology of mental health problems: a longitudinal population-based study. Journal of Child Psychology and Psychiatry. 2008 Jul;???-???
16. Egger HL, Angold A. Common emotional and behavioral disorders in preschool children: presentation, nosology, and epidemiology. Journal of Child Psychology and Psychiatry. 2006 Mar;47(3–4):313–37.
17. Ialongo NS, Rogosch FA, Cicchetti D, Toth SL, Buckley J, Petras H, et al. A Developmental Psychopathology Approach to Prevent Mental Health Disorders. In: Developmental Psychopathology. Hoboken, NJ, USA: John Wiley & Sons, Inc.; 2015. p. 968–1018.
18. Kovacs M, Goldston D. Cognitive and Social Cognitive Development of Depressed Children and Adolescents. J Am Acad Child Adolesc Psychiatry. 1991 May;30(3):388–92.
19. Muris P, Meesters C, van Melick M. Treatment of childhood anxiety disorders: a preliminary comparison between cognitive-behavioral group therapy and a psychological placebo intervention. J BehavTherExp Psychiatry. 2002 Sep;33(3–4):143–58.
20. Kingery JN, Erdley CA, Marshall KC, Whitaker KG, Reuter TR. Peer Experiences of Anxious and Socially Withdrawn Youth: An Integrative Review of the Developmental and Clinical Literature. Clin Child Fam Psychol Rev. 2010 Mar 13;13(1):91–128.
21. Birmaher B, Khetarpal S, Brent D, Cully M, Balach L, Kaufman J, et al. The Screen for Child Anxiety Related Emotional Disorders (SCARED): Scale Construction and Psychometric Characteristics. J Am Acad Child Adolesc Psychiatry. 1997 Apr;36(4):545–53.
22. Schiele MA, Domschke K. Trennungsangststörung. Nervenarzt. 2021 May 14;92(5):426–32.
23. Arab A, El Keshky M, Hadwin JA. Psychometric Properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED) in a Nonclinical Sample of Children and Adolescents in Saudi Arabia. Child Psychiatry Hum Dev. 2016 Aug 30;47(4):554–62.
24. Nigam AG, Marwah N, Goenka P, Chaudhry A. Correlation of general and dental anxiety in children aged 3 to 5 years: A clinical survey. J Int Oral Health. 2013 Dec;5(6):18–24.
25. Gale CK, Millichamp J. Generalised anxiety disorder in children and adolescents. BMJ Clin Evid. 2016 Jan 13;2016.
26. Layne AE, Bernat DH, Victor AM, Bernstein GA. Generalized anxiety disorder in a nonclinical sample of children: Symptom presentation and predictors of impairment. J Anxiety Disorder. 2009 Mar;23(2):283–9.
27. Alfano CA. Are Children With "Pure" Generalized Anxiety Disorder Impaired? A Comparison With Comorbid and Healthy Children. Journal of Clinical Child & Adolescent Psychology. 2012 Nov;41(6):739–45.
28. Wehry AM, Beesdo-Baum K, Hennelly MM, Connolly SD, Strawn JR. Assessment and Treatment of Anxiety Disorders in Children and Adolescents. Curr Psychiatry Rep. 2015 Jul 16;17(7):52.
29. Hjorthøj C, Stürup AE, McGrath JJ, Nordentoft M. Years of potential life lost and life expectancy in schizophrenia: a systematic review and meta-analysis. Lancet Psychiatry. 2017 Apr;4(4):295–301.
30. Wauthia E, Rossignol M. Emotional Processing and Attention Control Impairments in Children with Anxiety: An Integrative Review of Event-Related Potentials Findings. Front Psychol. 2016 May 3;7.
31. Orgilés M, Penosa P, Morales A, Fernández-Martínez I, Espada JP. Maternal Anxiety and Separation Anxiety in Children Aged Between 3 and 6 Years: The Mediating Role of Parenting Style. Journal of Developmental & Behavioral Pediatrics. 2018 Oct;39(8):621–8.
32. Buss KA. Which fearful toddlers should we worry about? Context, fear regulation, and anxiety risk. Dev Psychol. 2011 May;47(3):804–19.
33. Schwartz Ce, Snidman N, Kagan J. Adolescent Social Anxiety as an Outcome of Inhibited Temperament in Childhood. J Am Acad Child Adolesc Psychiatry. 1999 Aug;38(8):1008–15.
34. Chronis-Tuscano A, Degnan KA, Pine DS, Perez-Edgar K, Henderson HA, Diaz Y, et al. Stable Early Maternal Report of Behavioral Inhibition Predicts Lifetime Social Anxiety Disorder in Adolescence. J Am Acad Child Adolesc Psychiatry. 2009 Sep;48(9):928–35.
35. Beesdo K, Knappe S, Pine DS. Anxiety and Anxiety Disorders in Children and Adolescents: Developmental Issues and Implications for DSM-V. Psychiatric Clinics of North America. 2009 Sep;32(3):483–524.
36. Beesdo-Baum K, Winkel S, Pine DS, Hoyer J, Höfler M, Lieb R, et al. The diagnostic threshold of generalized anxiety disorder in the community: A developmental perspective. J Psychiatr Res. 2011 Jul;45(7):962–72.
37. Pine DS, Cohen P, Gurley D, Brook J, Ma Y. The Risk for Early-Adulthood Anxiety and Depressive Disorders in Adolescents with Anxiety and Depressive Disorders. Arch Gen Psychiatry. 1998 Jan 1;55(1):56.
38. Abad Mas L, Moreno Madrid P, VallsMonzó A, MartínezBorondo R, Ibáñez Orrico A, Mengodbalbas P, et al. Perception of anxiety and learning difficulties according to the criteria of the family and teachers of children with Attention Deficit Hyperactivity Disorder. Medicina Buenos Aires. 2023 Mar;83(2):17–21.
39. Leitenberg H, Gibson LE, Novy PL. Individual differences among undergraduate women in coping with stressful events: the impact of cumulative childhood stressors and abuse. Child Abuse Negl. 2004 Feb;28(2):181–92.
40. Ogden CL. Prevalence of High Body Mass Index in US Children and Adolescents, 2007-2008. JAMA. 2010 Jan 20;303(3):242.
41. Martinsen KD, Neumer SP, Holen S, Waaktaar T, Sund AM, Kendall PC. Self-reported quality of life and self-esteem in sad and anxious school children. BMC Psychol. 2016 Dec 13;4(1):45.
42. Ghandour RM, Sherman LJ, Vladutiu CJ, Ali MM, Lynch SE, Bitsko RH, et al. Prevalence and Treatment of Depression, Anxiety, and Conduct Problems in US Children. J Pediatr. 2019 Mar;206:256-267.e3.
43. Li WHC, Chung JOK, Ho KY, Kwok BMC. Play interventions to reduce anxiety and negative emotions in hospitalized children. BMC Pediatr. 2016 Dec 11;16(1):36.
44. Gale CK, Millichamp J. Generalised anxiety disorder in children and adolescents. BMJ Clin Evid. 2016 Jan 13;
45. Jiang Q, She X, Dill SE, Sylvia S, Singh MK, Wang H, et al. Depressive and Anxiety Symptoms among Children and Adolescents in Rural China: A Large-Scale Epidemiological Study. Int J Environ Res Public Health. 2022 Apr 20;19(9):5026.
46. James AC, Reardon T, Soler A, James G, Creswell C. Cognitive behavioral therapy for anxiety disorders in children and adolescents. Cochrane Database of Systematic Reviews. 2020 Nov 16;(11).
Received: 25 June 2023/ Accepted: 26 August 2023 / Published:15 September 2023
Citation: Roldán Bazurto M A, Montes-Escobar K, Zambrano Acosta J M, In-triago H M, Siteneski A. Anxiety levels and school performance of Ecuadorian children from 3 to 5 years old: a cross-sectional study. Revis Bionatura 2023;8 (3) 92 http://dx.doi.org/10.21931/RB/2023.08.03.92