2023.08.02.48
Files > Volume 8 > Vol 8 No 2 2023
Hemodynamic changes after repairing the congenital valvular heart disease

Hussein Togun 1,* , Munaf Ahmed 2, Zahraa Maan Majeed 1, Nisreen Alwaan1
, Munaf Ahmed 2, Zahraa Maan Majeed 1, Nisreen Alwaan1
1* Department of Biomedical Engineering, University of Thi-Qar, 64001 Nassiriya, Iraq
2 Al-Nasiriyah Heart Center Thi-Qar, 64001 Nassiriya, Iraq
1* Corresponding authors: *[email protected], [email protected]
Available from: http://dx.doi.org/10.21931/RB/2023.08.02.48
ABSTRACT
This paper studies hemodynamic changes after repairing congenital valvular heart disease. Two categories of Tetralogy of Fallot (TOF) and (ASD Primum) were collected from the Nasiriyah Heart Center between January 2015 and February 2022, with findings for 50 patients (28 patients with TOF & 22 patients with ASD Primum). The results showed that the spo2 value before the Surgery was low compared to its value after the Surgery, which was due to the existence of stenosis (obstruction) in the pulmonary artery; thus, the operations were undertaken to open the stenosis and return the percentage to normal. Because the patient with tetralogy of Fallot has stenosis in the pulmonary artery, compensatory found increases in the right ventricular diastolic pressure, and because the patient with tetralogy of Fallot has stenosis in the pulmonary artery, the PG value before the operation is more significant than after the operation. It was also discovered that the pG is exceptionally high due to stenosis (obstruction) in the pulmonary artery, which causes a drop in spo2. The findings demonstrated a link between age and MR before Surgery, with all patients between the ages of 2 and 47 suffering from Fatigue and restlessness. However, +++ denotes exhaustion and shortness of breath while not under stress, but ++ denotes Fatigue and shortness of breath when under normal stress.
Keywords: Artificial heart valve; Primum ASD; Tetralogy of Fallot; Mitral Valves 3.
INTRODUCTION
The heart is one of the most critical organs in the human body because it supplies blood to all body regions through a four-chamber system. In many developed countries, heart disease is the leading cause of mortality. Most heart diseases are caused by problems with the aortic and mitral valves (MV). Valvular repair is necessary to enhance the patient's quality of life and to consider symptom relief. Repairing a congenital valvular heart is a challenging surgical process, and several ways have been proposed. Surgical approaches vary depending on the underlying valve disease. The prevalence of all congenital aortic valve disorders is unknown due to a lack of data. Congenital aortic valve stenosis/obstruction of the left ventricular outflow tract (LVOT) was prevalent in 0.27–0.42 per 1,000 children 1,2. As more midterm and long-term series have been published over the last decade, the surgical approach to congenital mitral valve disease has progressed considerably 3, 4, 5. 6 presented aortic valve repair in children without a patch. Between 1980 and 2016, all children (n = 102) who underwent aortic valve replacement without using a patch were evaluated. The median patient age at the time of Surgery was 2 years (interquartile range, 1 month to 9.6 years). There were 17 newborns and 25 neonates. There were no surgical deaths. At ten years, the survival rate was 97.7% minus 0.01 percent (95 percent confidence interval, [CI] 91.0 percent -99.4 percent). There were 56 aortic valve reoperations in 43 patients (42.2%), comprising 24 redo aortic valve repairs, 22 Ross procedures, 8 mechanical aortic valve replacements, and 2 homograft aortic valve replacements. Aortic valve replacement could be accomplished without patches in around one-third of children who needed it. Aortic valve repair was accomplished in these youngsters without surgical mortality.
Stellin 7 conducted this study to determine whether the conservative surgical intervention of congenital MV abnormalities in the juvenile age group is usually advisable. The result of this therapy is preferable to MV replacement over 12 years. Between January 1987 and June 1999, thirty-four children (20 males and 14 females) with an average age of 5.9 years (range 45 days–18 years) were surgically treated for congenital MV disease. 4 patients (11.7%) were under the age of one year, and 21 patients (62%) were under the age of five years. Twenty-two individuals had MV incompetence (ubiquitous incompetence), whereas 12 had stenosis (or prevalent stenosis). In 22 cases, there were associated heart lesions (62.8 percent). The results suggest that MV reconstructive surgeries in newborns and children with congenital MV dysplasia are safe and successful, with low death and reoperation rates. Despite the common severity of MV dysplasia, mitral valve repair should always be tried, especially in newborns, to prevent the limitations of currently available prosthesis.
MATERIALS AND METHODS
Surgical Technique
These are the surgical techniques used during the surgical procedure for both cases. The following, Figure 1, has a flow chart explaining the general techniques used during Surgery. These techniques differ from one surgeon to another, one Center to another, and according to the patient's condition (damage).
Median sternotomy: is a type of surgical procedure in which a vertical inline incision is made along the sternum, after which the sternum itself is divided or "cracked." This procedure provides access to the heart and lungs for surgical procedures such as heart transplants, corrective Surgery for congenital heart defects, or coronary artery bypass surgery.
Cardio Pulmonary bypass: Its extracorporeal circuit provides physiological support in which venous blood is drained to a reservoir, oxygenated and sent back to the body using a pump.
Tetralogy of Fallot (TOF): A condition caused by a combination of four heart defects present at birth (congenital disabilities). These defects in the heart's structure cause oxygen-poor blood to flow from outside the heart to the rest of the body. The skin of infants and children with tetralogy of Fallot usually tends to be bluish because the blood does not carry enough oxygen.
An ostium primum atrial septal defect (ASD): Occurs when the atrial septum near the atrioventricular valves communicates between the two atrium, causing a left to right shunt and clefted anterior leaflet of mit. valve. This rarely develops into Eisenmenger's syndrome if pulmonary hypertension reverses the shunt's direction from right to left. Less common than the secundum type atrial septal defect, a primum ASD is usually small and less commonly requires intervention
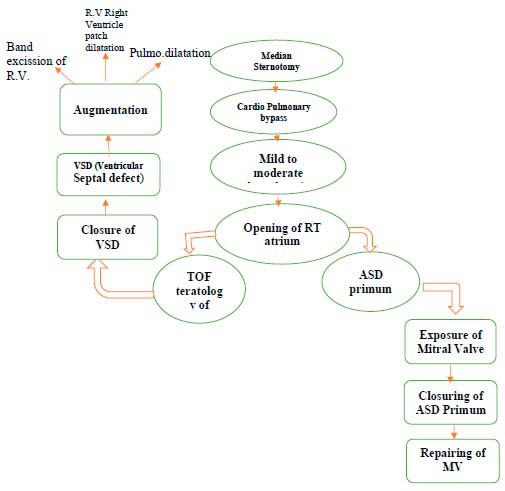
Figure 1. Surgical Technique.
Median sternotomy is a surgical procedure in which a vertical incision is made along the sternum, after which the sternum itself is divided or "cracked." This procedure provides access to the heart and lungs for surgical procedures such as heart transplants, corrective Surgery for congenital heart defects, or coronary artery bypass surgery.
Cardio Pulmonary bypass: Its extracorporeal circuit provides physiological support in which venous blood is drained to a reservoir, oxygenated and sent back to the body using a pump.
Tetralogy of Fallot (TOF): A condition caused by a combination of four heart defects present at birth (congenital disabilities). These defects in the heart's structure cause oxygen-poor blood to flow from outside the heart to the rest of the body. The skin of infants and children with tetralogy of Fallot usually tends to be bluish because the blood does not carry enough oxygen.
An ostium primum atrial septal defect (ASD): Occurs when the atrial septum near the atrioventricular valves communicates between the two atria causing a left to right shunt and clefted anterior leaflet of mit. valve. This rarely develops into Eisenmenger's syndrome if pulmonary hypertension reverses the shunt's direction from right to left. Less common than the secundum type atrial septal defect, a primum ASD is usually small and less commonly requires intervention.
RESULTS
In this paper, the study of hemodynamic changes after repairing congenital valvular heart disease with two categories, Tetralogy of Fallot (TOF) and Primum ASD, was conducted from January 2015 to February 2022 at the Nasiriyah Heart Center, where the results were for50 patients (28 patients with TOF & 22 patients with ASD Primum) the Table 1 shows a summary of the results of the TOF category and Table 2 shows a summary of the results of the Primum ASD category.
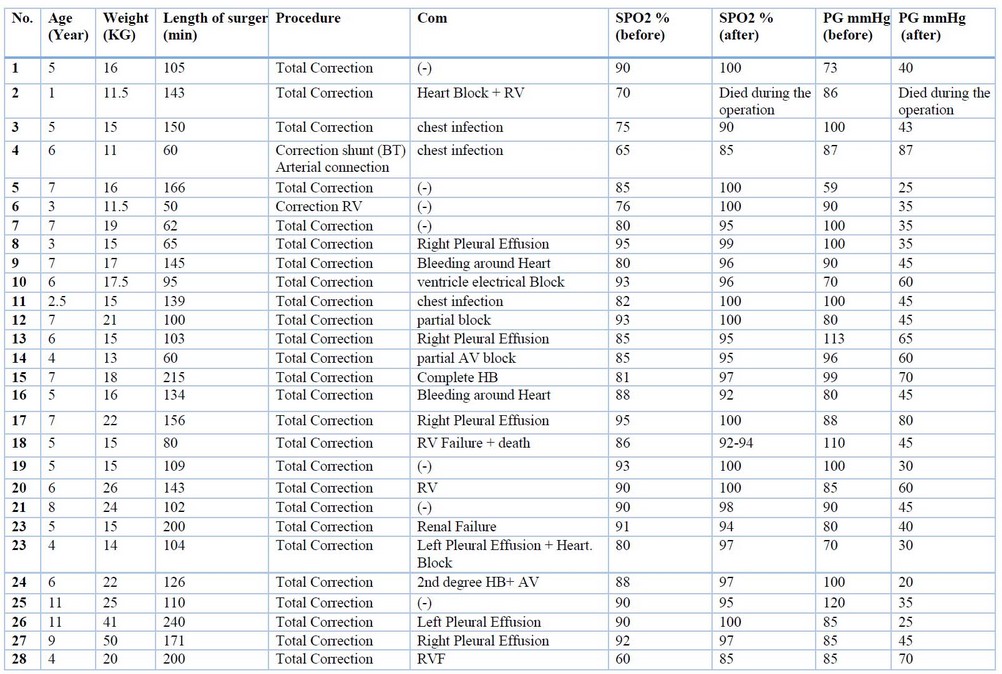
Table 1. Tetralogy of Fallot (TOF)
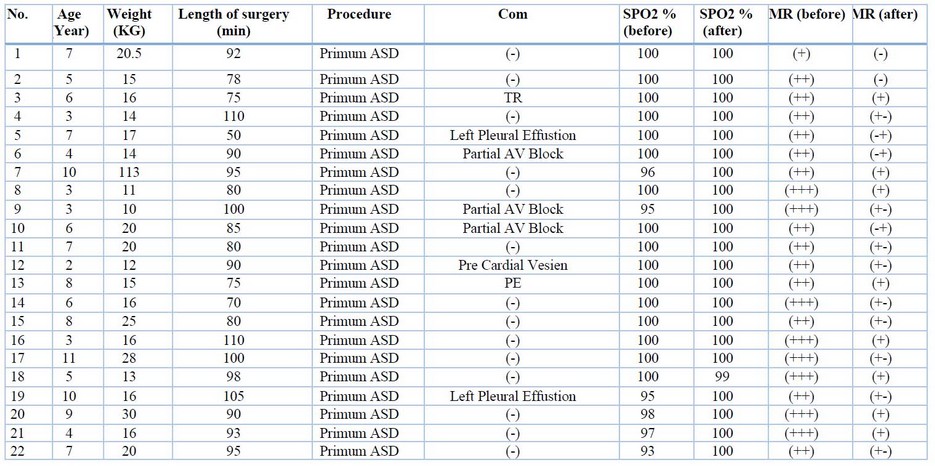
Table 2. Primum ASD.
Figure 2 shows the relationship between Spo2 before &After Surgery for the Tetralogy of Fallot, where the value of spo2 in normal people is (100-95) %. The results indicated that the value of spo2 before the Surgery is low compared to its value after the Surgery, and this is due to the presence of stenosis (obstruction) in the pulmonary artery, so the surgeries performed the operation and open the stenosis to make the percentage return to normal.
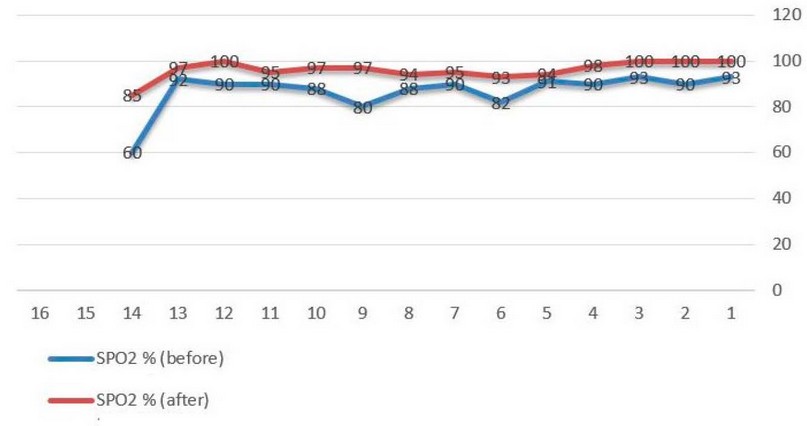
Figure 2. Relationship between PG Before & After Surgery
The Relationship between PG Before & After Surgery is presented in Figure 3. A pressure gradient (pG) across the pulmonary valve during right ventricular ejection, as seen in Figure 3. Compensatory discovered a rise in right ventricular diastolic pressure. Because the patient with tetralogy of Fallot has stenosis in the pulmonary artery, the PG value before the procedure is higher than after the operation. Furthermore, Figure 4 illustrated the relationship between PG & Spo2 before Surgery and found that the pG is very high due to the presence of stenosis (obstruction) in the pulmonary artery, which leads to a decrease in spo2.
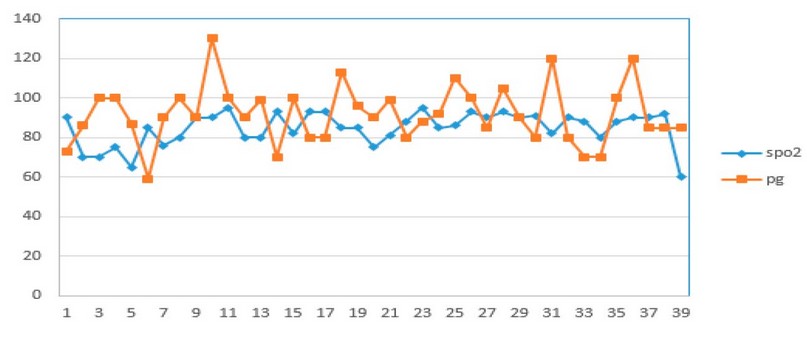
Figure 3. Relationship between PG & Spo2 Before Surgery
On the other hand, Figure 4 displays the relationship between PG & Spo2 after Surgery. In the case after the Surgery, it noticed an increase in spo2 by a large percentage, and it may return to its standard percentage due to removing the stenosis or blockage, which leads to a decrease in pG. In Figure 5 the results revealed that the relationship between Age& MR before Surgery was noted that all patients from the age of (1-11years) suffer from symptoms: Fatigue - restlessness. However, +++ refers to Fatigue and shortness of breath at rest, but ++ indicates Fatigue and shortness of breath when usual stress. Figure 6 noticed that in patients after the valve repair procedure, most of the patients had disappeared entirely symptoms and became normal. In contrast, others improved by a large percentage: where (+) indicates the patient's normal condition, while (+) indicates Fatigue and shortness of breath in case of intense stress.
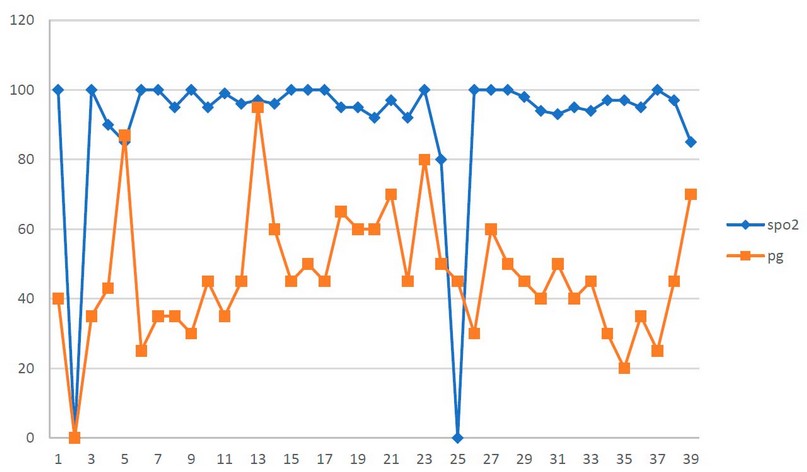
Figure 4. Relationship between PG & Spo2 After Surgery
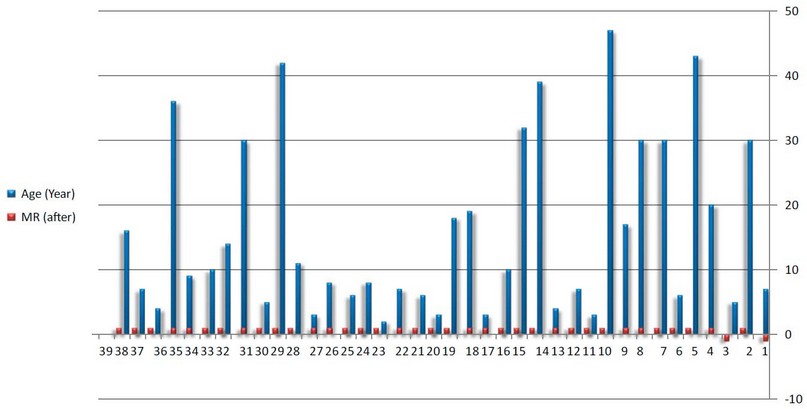
Figure 5. Relationship between Age& MR Before Surgery
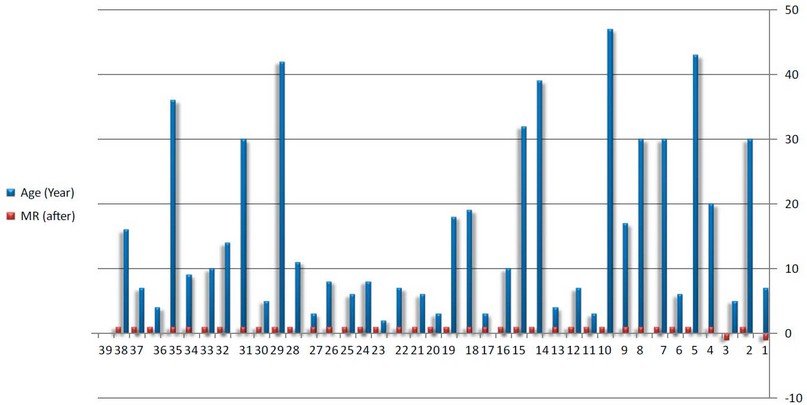
Figure 6. Relationship between Age& MR After Surgery
DISCUSSION
Abdulateef, S.M and Yuan, H 8,9 conducted research to assess MVR's long-term results. MVR in babies was performed using a personalized surgical technique that resulted in dependable valve performance and excellent survival. Although somatic development necessitates adjustment, the bi-leaflet mechanical prosthesis demonstrated adequate durability. This paper aims to study hemodynamic changes after repairing congenital valvular heart disease10,11.
CONCLUSIONS
The disease's congenital valvular repair is the focus of this study. The spo2 value before Surgery was low compared to its value after Surgery, which was linked to stenosis (obstruction) in the pulmonary artery; hence procedures to open the stenosis and restore the percentage to normal were conducted. Compensatory increases in right ventricular diastolic pressure were discovered in a patient with tetralogy of Fallot due to a constriction of the pulmonary artery. Why is there a poor relationship between age and weight in normal children? Due to a failure to thrive, as determined by the severity of the conclusion.
Author Contributions: Hussein Togun and Munaf Ahmed conceived of the presented idea. Hussein Togun developed the theory and performed the computations. Zahraa Maan Majeed and Nisreen Alwaan collected data and verified the analytical methods. All authors discussed the results and contributed to the final manuscript.
Data Availability Statement: Nasiriyah Heart Center is a medical center in Nasiriyah, Dhi Qar Governorate, Iraq, specializing in diagnosing and treating heart diseases such as ischemic heart disease, congenital heart defects, and valvular heart defects. The Center was opened on 10 July 2007; it employs a specialized staff of doctors, engineers and specialized medical and technical staff. The Nasiriyah Heart Center, consider the first place in southern Iraq in this rare specialty, is also an important step. In the transfer of strategic projects from the capital to the rest of the regions to provide medical and treatment services for heart patients in Dhi Qar Governorate and other governorates.
REFERENCES
1. Wu MH, Lu CW, Chen HC, et al. Adult Congenital Heart Disease in a Nationwide Population 2000-2014: Epidemiological Trends, Arrhythmia, and Standardized Mortality Ratio. J Am Heart Assoc 2018;7.
2. Marelli AJ, Mackie AS, Ionescu-Ittu R, et al. Congenital heart disease in the general population: changing prevalence and age distribution. Circulation 2007;72 115:163-72.
3. M.S. Uva, L. Galletti, F.L. Gayet, D. Piot, A. Serraf, J. Bruniaux, et al. Surgery for congenital mitral valve disease in the first year of life J Thorac Cardiovasc Surg, 109, 1995, pp. 164-174.
4. A. Serraf, J. Zoghbi, E. Belli, F. Lacour-Gayet, H. Aznag, L. Houyel, et al. Congenital mitral stenosis with or without associated defects: an evolving surgical strategy Circulation, 102 (19 Suppl 3) 2000, pp. III166-III171
5. E. Prifti, V. Vanini, M. Bonacchi, G. Frati, M. Bernabei, G. Giunti, et al. Repair of congenital malformations of the mitral valve: early and midterm results Ann Thorac Surg, 73, 2002, pp. 614-621
6. Fraser R O Wallace, Edward Buratto, Phillip S Naimo, Johann Brink, Yves d'Udekem, Christian P Brizard, Igor E Konstantinov, Aortic valve repair in children without use of a patch. J Thorac Cardiovasc Surg, 2021 Oct;162(4):1179-1189.
7. Stellin, G., Padalino, M., Milanesi, O., Vida, V., Favaro, A., Rubino, M., &Casarotto, D. Repair of congenital mitral valve dysplasia in infants and children: is it always possible? European journal of cardio-thoracic Surgery,2000 18(1), 74-82.
8. Abdulateef, S.M. ,O.K. Atalla, MQ. Al-Ani, TH. T. Mohammed, F.M. Abdulateef, O.M. Abdualmajeed , K. Mahmod. The effect of the electric shock on embryonic development and neurophysiological traits in the chick's embryo . IOP Conference Series: Earth and Environmental Science, 2021; 761(1), 012090.
9. Yuan, H., Wu, Z., Lu, T., Tang, Y., Chen, J., Yang, Y., & Huang, C. (2021). Long-term outcomes of mitral valve replacement in patients weighing less than 10 kg. Journal of Cardiothoracic Surgery, 2021, 16(1), 1-8.
10. AL- Shamary, W. A. .; Alkhateb, B. A. A. H. .; Abdel, E. T. . Role Of Perlite Quantity And Intervals Of Irrigation On Potatoes (Solanum Tuberosum L.) Grown In Gypsiferous Soil. Journal of Life Science and Applied Research. 2020, 1, 31-39.
11. Ohmayed, K. H. .; Sharqi, . M. M. .; Rashid, H. M. . Comparison Of The Physical And Chemical Changes In Local Organic Waste After Cultivation Of The Ganoderma Lucidum Mushroom And Composting By Common Methods. Journal of Life Science and Applied Research. 2020, 1, 1-9.
Received: May 15 2023/ Accepted: June 10 2023 / Published:15 June 2023
Citation: Togun, H.; Ahmed, M.; Majeed, Z.M.; Alwaan,N. Hemodynamic changes after repairing congenital valvular heart disease. Revis Bionatura 2023;8 (2) 48. http://dx.doi.org/10.21931/RB/2023.08.02.48