2021.06.03.8
Files > Volume 6 > Vol 6 No 3 2021
Comparison of Anxiety Levels in Patients with Coronavirus Disease (COVID-19) and their Families

Azin Chakeri 1 *, Maryam Rostami Qadi*2, Shima Haghani 3
Available from: http://dx.doi.org/10.21931/RB/2021.06.03.8
ABSTRACT
Very little research has been done on the anxiety of the families of patients with covid-19. Considering the vital role of the family in the continuation of supportive-psychological therapies and the direct impact on the patient's anxiety level, in this study, we examined the anxiety level of the family of patients with Covid-19 and compared their with their patient's anxiety level. In this comparative study, the samples were 60 people who were given a definitive diagnosis of covid-19 in selected hospitals (Masih Daneshvari Hospital and Besat Hospital). From the family members, the person who, according to the patient, is most affected and has an emotional relationship with him (spouse-father-mother-child) was selected. The standard Spielberger Anxiety Questionnaire has been used to measure apparent (state) and hidden (trait) anxiety. The questionnaire was completed by both groups (patient-family) and compared with each other. The mean of evident anxiety in patients and caregivers was 70.82 and 74.2, respectively, which this difference was statistically significant (P = 0.023). It is also observed that the mean of hidden anxiety in patients and caregivers was 68.83 and 74.71, respectively, which the mean of hidden anxiety in patients was significantly less than caregivers (P = 0.006). After identifying anxiety, nurses can better and more effectively deal with these unwanted conditions in the patient and her family by providing appropriate and correct education.
Keywords: Anxiety, COVID-19, Patient.
INTRODUCTION
In December 2019, a viral outbreak was reported in Wuhan, China. The cause of this disease was a new and genetically modified virus from the family of coronaviruses called SARS-COV, which was named Covid-19 disease1. Unfortunately, due to its very high prevalence, the virus spread rapidly throughout the world and infected almost all world countries in a short period (less than four months) 2, 3. The COVID-19 virus has spread easily in some affected areas of the community. The local spread of COVID-19 disease means that individuals are infected in this region. Some individuals are not sure how or where they became infected4. COVID-19 virus is developed quickly in diverse parts of Iran and instigated people to different levels of anxiety. The symptoms of this virus vary from mild to severe. Signs and symptoms of infection include fever, cough, and breathing difficulty5. Anxiety is a common sign in patients suffering from respiratory disorders and can significantly reduce patients' quality of life. The majority of the anxiety cases develop clinical symptoms associated with severe respiratory disease and side effects of medications6. Lung diseases, including pulmonary disorders, are highly associated with anxiety disorders. Illness with severe clinical signs and also duration caused more levels of anxiety7.
Higher distribution of anxiety and depression in lung diseases has been reported compared to other cases. The previous survey showed that 20-40% of patients who suffered from Chronic Obstructive Pulmonary Disease (COPD) had symptoms of anxiety8. In a study of patients with asthma and COPD, Pietras et al. found a positive association between anxiety and dyspnea9. Clinical anxiety affects up to two-thirds of chronic respiratory patients and reduces the quality of life and physical function. Little research has been done on anxiety experiences in patients with severe respiratory symptoms10. Anxiety is common in cases of COVID-19 and appears to be due to the unknown and cognitive ambiguity of the virus. Anxiety caused a severe reduction in the immunity levels of humans has always been anxious for human11. At this time, people are looking for more information to relieve their anxiety. Anxiety can make people unable to distinguish right from wrong to be exposed to false news. Stress and anxiety can weaken the immune system and make them vulnerable to diseases such as Coronavirus12.
Anxiety is a psychological condition that almost all human beings experience to varying degrees throughout their lives. But when it increases and reaches a level that causes distress and conflict, it is known as a disorder. Anxiety disorder is one of the most common disorders characterized by persistent, excessive, and unrealistic concerns about everyday issues13. This disorder can cause sleep problems, centralization, physical problems such as; burnout, headaches, tension, muscle pain, and many problems in the future for people14. Evidence shows that this disorder is more common in people who had crises in their lives. Li et al. conducted a study to investigate the psychological consequences of COVID-19 in China through an online survey and concluded that the disease increased anxiety, stress, and decreased happiness among people. Given the global (pandemic) status of Covid-19 disease, which affects almost all essential economic, political, social, and even military aspects of all countries of the world, in other words, paralyzed, the psychological effects of this viral disease on mental health is very important for people at different levels of society15. Due to this virus's pathogenicity, spread rate, and high mortality rate, individuals' mental health status, including patients, health care workers, families, children, students, psychiatrists, and staff of various occupations, may be endangered16, 17. It is essential to pay attention to this fact that in connection with the observance of protocols and training given to patients to reduce anxiety, the family plays a decisive and vital role. The family is the context of each person who plays a crucial role in guiding him.
Effective communication between the treatment team and the patient's family members is critical to provide safe care and prevent further injury to the patient18. This is especially important for providing quality care services in stressful and unknown diseases such as Covid-19. Infection of one member of the family with this disease causes anxiety and psychological problems in other family members. Therefore, it is necessary to know the level of anxiety in patients' families due to their direct impact on increasing or decreasing the level of patient's anxiety and follow-up and continuation of supportive therapies19. When a patient enters the emergency department, the patient's family usually experiences psychological conditions such as anxiety and worry, such as fear or response to an unknown threat, which is a general reaction to stressful situations such as illness or life-threatening situations20. The patient's family members play an essential role in supporting the patient and cause the desired therapeutic response in the patient. However, when anxiety is high in family members, they may not play an effective supportive role21. Very little research has been done on the anxiety of the families of patients with covid-19. Considering the vital role of the family in the continuation of supportive-psychological therapies and the direct impact on the patient's anxiety level, in this study, we examined the anxiety level of the family of patients with Covid-19 and compared their with their patient's anxiety level.
METHODS
Participants
This study was a comparative study. The research environment of this study included the emergency departments of selected hospitals for admission of patients with covid-19 (Masih Daneshvari Hospital and Besat Hospital). The study samples consisted of 60 people (men and women) who were given a definitive diagnosis of covid-19 by performing a corona test with a CT scan of the lungs, and the treating physician quarantined them at home and received medication and continued treatment at home with their family, which were selected by continuous sampling from the research environment. From the family members, the person who, according to the patient, is most affected and has an emotional relationship with him (spouse-father-mother-child) was selected.
Data collection tools
The questionnaire used to collect data in this study consists of two parts. The first part was a researcher-made questionnaire containing demographic information (age, level of education, marital status, and occupation). The second part was the standard Spielberger Anxiety Questionnaire, which showed patients' current level of anxiety and their families. This questionnaire has been used extensively in research and clinical practice and includes separate self-assessment scales to measure obvious and hidden anxiety. The questionnaire has been translated into 30 languages of the world and has been adapted to Iranian culture, in other words, it has been standardized22. Mehram, in 1373 calculated the reliability of this test through Cronbach's alpha on the average population (=0.9452). In general, scores (20-42) of mild anxiety, scores (43-64) of moderate anxiety, and scores (65-80) are classified as severe anxiety23.
Data collection
All samples of the study that met the inclusion criteria (corona test and positive lung scan) were selected by continuous sampling with a selected person from their family (responsible for patient care) informed consent to participate in the study researcher. Then the standard Spielberger anxiety questionnaire was completed by both groups (patient-family) and compared with each other.
RESULTS
The results showed that the mean age of the patients was 43.25 with a standard deviation of 11.18 years, and 76.7% of them were married, and the educational level was 36.7% at the diploma level. The mean age of the caregiver was 42.8 years with a standard deviation of 10.77 years, and 80% of them were married, and the educational level was 40% at the bachelor level (Table 1).
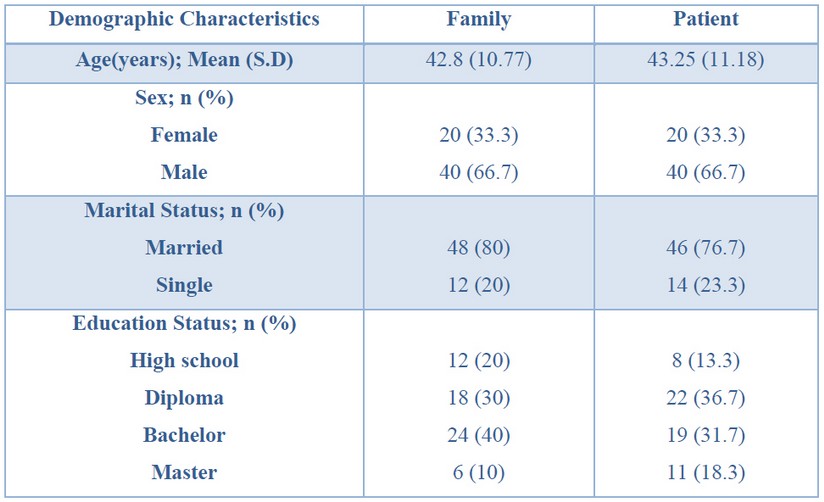
Table 1. Frequency Distribution of Demographic Characteristics of the Participants.
Table 2 shows that none of the patients and their caregivers had apparent (state) anxiety at a superficial level, and the apparent anxiety of all caregivers and 98.3% of patients was high. The mean of evident anxiety in patients was 70.82 with a standard deviation of 7.59, and the mean of evident anxiety in caregivers was 74.2 with a standard deviation of 4.24. Based on the result of the Kruskal-Wallis test, this difference was statistically significant, and the mean of evident anxiety of patients was significantly less than caregivers (P = 0.023). It is also observed that all caregivers' hidden (trait) anxiety was high, and 88.4% of patients had hidden anxiety at a high level. The mean of hidden anxiety in caregivers was 74.71 with a standard deviation of 2.91 and in patients was 68.83 with a standard deviation of 10.72. Based on the result of the Kruskal-Wallis test, this difference was statistically significant, and the mean of hidden anxiety in patients was significantly less than caregivers (P = 0.006).

Table2. Frequency Distribution of Anxiety of the Participants.
DISCUSSION
COVID-19 is a pandemic disease with high mortality rates and distribution globally24-27. In this study, it was found that this disease (COVID-19) is anxious for most patients and causes more anxiety in the family (patient caregivers) than the patient. The mean of state anxiety in patients was 70.82, and the mean of state anxiety in caregivers was 74.2. Also, the mean of trait anxiety in patients was 68.83, and this means in caregivers was 74.71. Given the importance of the role of the family in the treatment of patients, and considering that most of the educational programs related to corona in medical centers are held only for patients, this study recommends that in addition to the patient, appropriate educational programs should also be considered for their family. The most appropriate providers of education in hospital wards are the nurses of such wards, who, in addition to frequently encountering similar patients and their families, also have the most time to communicate with them28. After identifying anxiety, nurses can better and more effectively deal with these unwanted conditions in the patient and her family by providing appropriate and correct education29,30.
CONCLUSION
This research showed that the COVID-19 pandemic diseases caused severe effects on patients and their families mental and nervous systems. The majority of cases were faced with apparent anxiety. As anxiety in COVID-19 patients and their families may cause weakening of mood, despair, and hopelessness and finally encouraging the patient not to fail the disease; thus, it is essential to use antidepressant therapeutic agents to reduce the rate of anxiety among patients and their families. This is the first report comparing anxiety levels in patients with Coronavirus Disease (COVID-19) and their families globally. Thus, further investigations should perform to find more aspects of the COVID-19 mental disorders.
REFERENCES
[1] Zhu, H., Wei, L. and Niu, P. 2020. The novel coronavirus outbreak in Wuhan, China. Global Health Research and Policy, 5(1), 1-3.
[2] Remuzzi, A. and Remuzzi, G. 2020. COVID-19 and Italy: what next? Lancet (London, England).
[3] Zangrillo, A., Beretta, L., Silvani, P., Colombo, S., Scandroglio, A. M., Dell'Acqua, A., Fominskiy, E., Landoni, G., Monti, G. and Azzolini, M. L. 2020. Fast reshaping of intensive care unit facilities in a large metropolitan hospital in Milan, Italy: facing the COVID-19 pandemic emergency. Critical Care and Resuscitation, 22(2), 91.
[4] Jernigan, J. A., Low, D. E. and Helfand, R. F. 2004. Combining clinical and epidemiologic features for early recognition of SARS. Emerging Infectious Diseases, 10(2), 327.
[5] Wu, Z. and McGoogan, J. M. 2020. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA, 323(13), 1239-1242.
[6] Dong, X.-Y., Wang, L., Tao, Y.-X., Suo, X.-l., Li, Y.-C., Liu, F., Zhao, Y. and Zhang, Q. 2017. Psychometric properties of the Anxiety Inventory for Respiratory Disease in patients with COPD in China. International Journal of Chronic Obstructive Pulmonary Disease, 12, 49-58.
[7] Cassem, N. and Bernstein, J. 2004. Depressed Patients (5th ed.). Philadelphia, PA: Mosby/Elsevier.
[8] Coventry, P. A. 2009. Does pulmonary rehabilitation reduce anxiety and depression in chronic obstructive pulmonary disease? Current Opinion in Pulmonary Medicine, 15(2), 143-149.
[9] Pietras, T., Witusik, A., Panek, M., Hołub, M., Gałecki, P., Wujcik, R. and Górski, P. 2009. Anxiety and depression in patients with obstructive diseases. Polski Merkuriusz Lekarski: Organ Polskiego Towarzystwa Lekarskiego, 26(156), 631-635.
[10] Willgoss, T. G., Goldbart, J., Fatoye, F. and Yohannes, A. M. 2013. The development and validation of the anxiety inventory for respiratory disease. Chest, 144(5), 1587-1596.
[11] Alipour, A., Ghadami, A., Alipour, Z. and Abdollahzadeh, H. 2020. Preliminary validation of the Corona Disease Anxiety Scale (CDAS) in the Iranian sample.
[12] Al-Rabiaah, A., Temsah, M.-H., Al-Eyadhy, A. A., Hasan, G. M., Al-Zamil, F., Al-Subaie, S., Alsohime, F., Jamal, A., Alhaboob, A. and Al-Saadi, B. 2020. Middle East Respiratory Syndrome-Corona Virus (MERS-CoV) associated stress among medical students at a university teaching hospital in Saudi Arabia. Journal of Infection and Public Health, 13(5), 687-691.
[13] Yu, W., Singh, S. S., Calhoun, S., Zhang, H., Zhao, X. and Yang, F. 2018. Generalized anxiety disorder in urban China: Prevalence, awareness, and disease burden. Journal of Affective Disorders, 234, 89-96.
[14] Rijn, B. v. and Wild, C. 2013. Humanistic and integrative therapies for anxiety and depression: Practice-based evaluation of transactional analysis, gestalt, and integrative psychotherapies and person-centered counseling. Transactional Analysis Journal, 43(2), 150-163.
[15] Li, S., Wang, Y., Xue, J., Zhao, N. and Zhu, T. 2020. The impact of COVID-19 epidemic declaration on psychological consequences: a study on active Weibo users. International Journal of Environmental Research and Public Health, 17(6), 2032.
[16] Bao, Y., Sun, Y., Meng, S., Shi, J. and Lu, L. 2020. 2019-nCoV epidemic: address mental health care to empower society. The Lancet, 395(10224), e37-e38.
[17] Chen, Q., Liang, M., Li, Y., Guo, J., Fei, D., Wang, L., He, L., Sheng, C., Cai, Y. and Li, X. 2020. Mental health care for medical staff in China during the COVID-19 outbreak. The Lancet Psychiatry, 7(4), e15-e16.
[18] Dawood, E., Misuta, R., Alharbi, M., Almurairi, A., Kanori, H. and Alsaiari, M. 2018. Relationship between Nurses' Communication and Levels of Anxiety and Depression among Patient's Family in the Emergency Department. Ann Psychiatry Ment Health, 6(1), 1125.
[19] Hosieni, F., Ravari, A. and Akbari, A. 2017. The Effect of Communicating with Patients Using Peplau Model on Patients' Satisfaction with the Provided Nursing Cares at the Cardiac Intensive Care Unit. Iran Journal of Nursing, 29(104), 36-45.
[20] Townsend, M. and Morgan, K. 2017 Psychiatric mental health nursing: Concepts of care in evidence-based practice. FA Davis.
[21] Zarei, M., Keyvan, M. and Hashemizadeh, H. 2015. Assessing the Level of Stress and Anxiety in Family Members of Patients Hospitalized in the Special Care Units. International Journal of Review in Life Sciences, 5(11), 118-122.
[22] Basam pour, S. 2004. The effect of preoperative training on the anxiety level of patients undergoing open heart surge. Payesh Journal, 2, 139-144.
[23] Behrouz, m. 1994. Spielberger anxiety test norms in mashhad. M.SC Allameh Tabatabai University.
[24] Ranjbar R, Mahmoodzadeh Hosseini H, Safarpoor Dehkordi F. A Review on Biochemical and Immunological Biomarkers used for Laboratory Diagnosis of SARS-CoV-2 (COVID-19). The Open Microbiology Journal. 2020;14(1).
[25] Mirzaie A, Halaji M, Dehkordi FS, Ranjbar R, Noorbazargan H. A narrative literature review on traditional medicine options for treatment of corona virus disease 2019 (COVID-19). Complementary Therapies in Clinical Practice. 2020:101214.
[26] Halaji M, Farahani A, Ranjbar R, Heiat M, Dehkordi FS. Emerging coronaviruses: first SARS, second MERS and third SARS-CoV-2: epidemiological updates of COVID-19. Infez Med. 2020;28(suppl 1):6-17.
[27] Sheikhshahrokh A, Ranjbar R, Saeidi E, Dehkordi FS, Heiat M, Ghasemi-Dehkordi P, Goodarzi H. Frontier therapeutics and vaccine strategies for sars-cov-2 (COVID-19): A review. Iranian Journal of Public Health. 2020;49:18-29.
[28] Arrebola‐Pajares, A., Tejido‐Sanchez, A., Jimenez‐Alcaide, E., Medina‐Polo, J., Perez‐Cadavid, S., Guerrero‐Ramos, F. and Diaz‐Gonzalez, R. 2014. Survey of satisfaction in hospitalized patients at a urology department. Archivos Espanoles De Urologia, 67(7), 621–627.
[29] Brunner, L., Smeltzer, S., Bare, B., Hinkle, P. and Cheever, K. 2017. Brunner & Suddarth's textbook of medical‐surgical nursing. Philadelphia: PA: Williams & Wilkins.
[30] Dehkordi FS, Valizadeh Y, Birgani TA, Dehkordi KG. Prevalence study of Brucella melitensis and Brucella abortus in cow's milk using dot enzyme linked immuno sorbent assay and duplex polymerase chain reaction. J Pure Appl Microbiol. 2014;8(2):1065-9.
Received: 15 April 2021
Accepted: 20 May 2021
Azin Chakeri 1 *, Maryam Rostami Qadi*2, Shima Haghani 3
1. Correspond author, Department of Nursing, Garmsar branch, Islamic Azad University, Garmsar, Iran.
Email:[email protected].
2. Department of nursing sari bu-Ali sina Therapeutic and Education center Mazandaran University of medical science, Sari, Iran.
3. Master of Biostatistics, Nursing Care Research Center, Iran University of Medical Sciences, Tehran, Iran.
Corresponding author: Maryam Rostami Qadi, Email: [email protected]