2023.08.02.28
Files > Volume 8 > Vol 8 No 2 2023
Relationship between Toll-like Receptors and Pathogenesis of Systemic Lupus Erythematosus

Basma Ahmed Ratib1* , Asmaa Mohammed Saud1
, Asmaa Mohammed Saud1
1 Institute of genetic engineering and Biotechnology for postgraduate studies, University of Baghdad;basima @ige.uobaghdad.edu.iq
2 Institute of genetic engineering and Biotechnology for postgraduate studies, University of Baghdad;[email protected]
* Correspondence: basima @ige.uobaghdad.edu.iq
Available from: http://dx.doi.org/10.21931/RB/2023.08.02.28
ABSTRACT
Systemic Lupus Erythematosus is a chronic inflammatory disease characterized by a loss of self-antigen tolerance and the development of high titers of serum autoantibodies, with a wide range of clinical manifestations and complex etiologies. Its etiology is influenced by various genetic, hormonal, immunologic, and environmental factors. SLE affects around 90% of women of reproductive age. The study aims to evaluate the serum levels of Toll-like receptor 7 (TLR7) in a sample of Iraqi SLE patients and its potential relationship with other clinical and laboratory parameters. The study included 100 female patients and 50 healthy females with an age range of (16-65) years old and healthy individuals with an age range of (16-65) years old and mean ages of (35.72 ±11.66 and 35.72 ±11.66) respectively. The current study is performed to estimate the serum levels of (TLR7, ANA, Urea, creatinine, and Vitamin D3) and a laboratory investigation for ESR, hemoglobin, and white blood cells by using the enzyme-linked immunosorbent assay (ELISA)and automated Fujifilm. Serum levels of TLR7 were increased in the SLE patients compared to the control, and a significant difference has been observed (P≤0.01) among SLE patients compared to the control. Urea, creatinine, and ESR were significantly higher; at the same time, the Vitamin D3, hemoglobin, and white blood cells were significantly lower (p< 0.01) among SLE patients as compared to control. On the other hand, there was no evidence of any correlation between TLR7 serum level and disease laboratory investigation.
Keywords: Antinuclear autoantibody, Haemoglobin, Interferon, SLE, Toll-Like Receptor-7, WBC.
INTRODUCTION
Systemic lupus erythematosus (SLE) is a systemic autoimmune disease characterized by multisystemic and multi-organ involvement. The presence of numerous autoantibodies that induce the development and deposition of immune complexes as well as other immunological processes is related to the symptoms of SLE 1. The mechanisms underlying this disease are complicated and unknown, but they are thought to be linked to environmental activation of the body's immunological dysfunction and defective immune regulation 2. Antinuclear antibody (ANA), anti-double-stranded DNA antibodies, complement 3 protein (C3), complement 4 protein (C4), and leukopenia are among the few indicators that help physicians make decisions on disease diagnosis and prognosis 3. Human plasmacytoid dendritic cells (pDCs) are thought to be essential contributors to the development of autoimmune disorders, SLE; they can produce cytokines and chemokines in response to autoimmune complexes such as self-DNA and small nuclear ribonucleoprotein particles (snRNPs). TLR7 had a higher expression on human pDCs than the other TLRs. Continuous stimulation of pDCs by endogenous nucleic acids activates SLE's type I IFN system, resulting in prolonged type I IFN production. TLR7 and TLR9 are associated with B cell activation and IFN- production in SLE 4,5. B cell abnormalities are crucial in developing systemic lupus erythematosus (SLE) 6. Both central and peripheral tolerance mechanisms inhibit the growth and survival of B lymphocytes that react to self-antigens 7. When these tolerance mechanisms fail, autoreactive B cells are produced, contributing to SLE's pathogenesis. TLRs, which sense nucleic acids in endosomes, are responsible for the cell-intrinsic loss of B cell tolerance to autoantigens in people with SLE. TLR7 drives the extrafollicular B cell response and the germinal center reaction, which are involved in autoantibody production and disease pathogenesis. Autoreactive B cells identify DNA-associated antigens (such as unmethylated cytosine-phosphate-guanosine (CpG) motifs) and RNA-associated antigens (such as the single-stranded RNA (ssRNA) short nuclear RNA, U11) in systemic lupus erythematosus (SLE). These self-antigens are thought to be released due to dysregulated pathways that cause an increase in neutrophil extracellular traps (NETs), necrotic cells, or apoptotic cells 8. The B cell receptor (BCR) recognizes these autoantigens on the surface of B cells and triggers their cellular internalization. Once within the endosomes, In B lymphocytes, self-antigens can activate Toll-like receptor 7 (TLR7) and TLR9. TLR7 expression is greater in women than in men because TLR7 is located on X chromosome 9,10. The TLR7 gene escapes X-chromosome inactivation, resulting in considerably higher amounts of TLR7 protein than in male cells 11. Genetic or environmental factors contributing to TLR7 overexpression enhance an individual's sensitivity to SLE (such as gender, nutrition, and cytokine media, especially the amount of type I interferons) 8. In physiological circumstances, TLR9 inhibits TLR7 signaling, and this chemical protects people from developing SLE. TLR9 function disruption, on the other hand, may favor TLR7 signaling and contribute to the development of SLE 8. This study aims to assess the relationship between serum levels of TLR7 and clinical and laboratory indicators in Iraqi female patients with SLE.
MATERIALS AND METHODS
Subject
After obtaining the approval of the Ethics Committee in the Biotechnology Department, College of the Science ‚ University of Baghdad, the peripheral blood samples were collected from all participants of 100 SLE patients. Informed consent was obtained from all participants before their inclusion in the study. All SLE patients met the American College of Rheumatology 12 classification criteria.
Inclusion and Exclusion criteria
We used available data to apply typical inclusion criteria for SLE, including the age of (16-65) years and a positive SLE EULAR/ACR 12 diagnosis. Patients with other immunological disorders or overlapping autoimmune diseases and patients with juvenile SLE (early-onset) who were less than 16 years old were excluded from the study.
Laboratory Investigations
The laboratory tests were conducted to evaluate the immunological and routine tests. The patients and controls were tested for total serum levels of TLR-7 as well as antinuclear autoantibody (ANA), complete blood count (CBC), Erythrocyte sedimentation rate (ESR), Vitamin D3 (25(OH)D), blood urea and creatinine levels. Blood (3 ml) was withdrawn from each subject (patients and controls), divided into sterile gel tubes, and left for about two hours to clot. The sample was then centrifuged at 3000 rpm for 15 minutes to separate the serum stored at -20°C until assayed. ELISA kits were employed to assess levels of total TLR-7(BioSource Inc, British) and ANA 13. The blood urea and creatinine levels were measured using an automated Fujifilm. Two milliliters of venous blood were withdrawn from each subject by vein puncture under an aseptic technique with a multi-sample syringe. To estimate the complete blood count, whole blood was placed in EDTA tubes and tested by a Hematology analyzer.
Toll-Like Receptor-7 Measurement
The serum level of TLR-7 titer was measured using the ELISA technique and commitment to the instructional manual provided by manufacturer BioSource Inc, British (Cat. No RDEEH2015).
Statistical analysis
SPSS software (Statistical Package for the Social Sciences) version-13 was used to analyze the subjects' data to determine the effect of different components in research parameters. Parametric results (quantitative) were used to compute TLR7 levels, whereas non-parametric data (qualitative) was calculated using means and standard deviation. Additionally, the Pearson Chi-square test was utilized for comparisons, and the Spearman correlation was used to test the correlation between different study parameters if the P-value is considered significant if it is less than 0.05 14.
RESULTS
The number of Systemic Lupus Erythematosus patients selected for the current study was 100 of SLE patients and 50 healthy control individuals; all participants in this study were female. The age range of SLE patients was between 16 to 65 years, with a mean and standard deviation value equal to (35.72 ± 11.66 years). The age range of the controls was identical to the age range of patients (34.05 ± 11.02 years). The participants were divided into ages 16-29, 30-49 and > 50 years. The percentage of the SLE patient in the same age groups was (36.00%, 54.00%, and 10.00%), respectively. While the rate of healthy subjects for the same age groups was (42.00%, 48.00%, and 10.00%), respectively. as shown in Table 1.

Table 1. Distribution of subjects according to age and age group.
One of the essential parameters in SLE diagnosis is the serum level of total TLR-7. Table 3 shows the average concentration level of total TLR-7 in the serum of SLE patients compared to that of the control. The total TLR-7 mean level of the systemic lupus group (4.68 ±1.65) was higher than that of the control group (1.86 ±0.41), with a highly significant difference (P=0.0001), as shown in Table 2.

Table 2. TLR7 level of systemic lupus erythematosus patients in comparison with controls.
All the laboratory tests of the female SLE patients and healthy control enrolled in this study were described in Table 3. There was a significant difference in Urea, creatinine, ANA, and ESR were significantly higher; at the same time, the Vitamin D3, hemoglobin, and white blood cells were significantly lower among SLE patients as compared to control
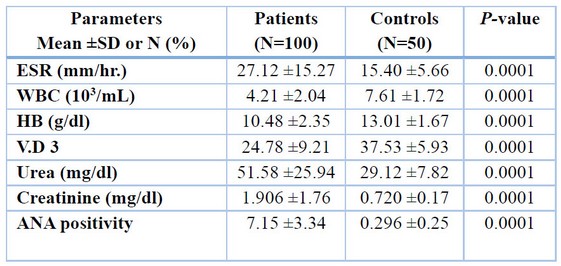
Table 3. Laboratory investigations in all studied groups.
Values are expressed as N: number in each parameter, %: percentage in each group and mean ± SD. The abbreviations are; WBC: white blood cell, Hb: hemoglobin, S: serum, V.D3: vitamin D3, ANA: antinuclear antibody. Normal ranges: WBCs (109/L), 4.00-10.00; HB (g\dl), 150-450; urea (mg\dl), 15-45; Creatinine (mg\dl), 0.3-0.7, V.D3: (ng/ml), 30-50. *Correlation is significant at the 0.05 level (2-tailed)
Personal correlation between TLR-7 levels and laboratory parameters, including ANA, WBC, Hb, ESR, Urea, creatinine, and Vit.D3, statistically show an insignificant correlation with TLR7 according to laboratory examinations, as shown in Table 4.
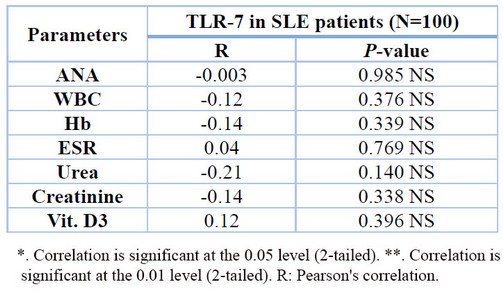
Table 4. Correlations between TLR-7 and laboratory parameters.
DISCUSSION
Systemic lupus erythematosus is a multisystemic autoimmune disease with a wide range of clinical manifestations and a high risk of morbidity and mortality 15. SLE is characterized by an increased production of autoantibodies directed against self-antigens, a wide range of clinical symptoms, and an entirely unpredictable flare-up course 16. Due to the low prevalence of the disease in males, all the studied group were females; due to different hormonal secretions between males and females, SLE primarily affects women in their reproductive years and affects any organ in the body 17, estrogen and prolactin (sex hormones associated with female reproduction and development) higher levels of these hormones can allow more B cells to circulate in the body. Next, the increased level of B cells can lead to an immune response and may trigger symptoms of SLE, and this can be attributed to a risk factor for female gender and age in the genesis of SLE. Concerning age, SLE is thought to be a disease that affects middle-aged individuals more than younger or older persons. The recorded age of this study ranged from 16 to 65 years with a mean age of (35.72years). These results correspond with 18 studies documenting SLE Iraqi patients' peak range between <20 to >50. The current study showed that the thirtieth decade is regarded as a critical risk factor; this is in agreement with 19, who showed that The most susceptible age for SLE is 20–39 years for females. Women were more frequently affected than men for every age and ethnic group 20. The current study applied SLE cases to females of different ages; most studies agree that females are affected at considerably higher rates than males 21. Sex hormones affect immunological responses and modulate molecular pathways in the innate and adaptive immune systems 22. Women's higher rates of SLE may be due to endogenous estrogen, X chromosomal inactivation failures, increased Toll-like receptor gene products, and alterations in microRNA activity, among other factors 23.
Human SLE has been associated with TLR7 overexpression 24. In the current study, there was a significant difference in mean TLR7 serum levels between SLE patients (4.68 ±1.65) and healthy controls (1.86 ±0.41), so (P= 0.0001). This is because TLR7 produces type I interferon and promotes the activation of autoreactive B lymphocytes 25. This study showed a significant increase in the serum level of TLR7 in SLE patients; this result was supported by 26 who showed that total TLR-7 (p<0.01) levels were significantly increased in lupus patients compared to age-matched controls.
Antinuclear antibodies (ANA) more specific autoantibody testing may be helpful in the diagnosis of suspected SLE or ANA-associated disease 27. Also, it is discussed as an entrance criterion for SLE, while the number of ANA-negative patients worldwide is small (>5%) 28. Evidence suggests that ANA responses can deteriorate over time due to disease progression or medication side effects 29. The current study finds that ANA positivity of 98% in SLE patients, as a result, shows a significant difference in the mean of ANA serum levels between SLE patients and healthy controls, however, these results correspond with 30 studies on Iraqi SLE patients who recorded ANA test:98%. Also, ANA shows an insignificant correlation with TLR7. This disagrees with 31, who reported that TLR7 ligand stimulation in SLE patients resulted in antinuclear autoantibodies (ANA) production.
Evidence suggested that Vitamin D3 could exert some of its immunomodulatory effects in SLE patients by affecting the expression levels of some TLRs 32. Vitamin D3 in the current study shows an insignificant correlation with TLR7. In contrast, it offers a significant difference in the mean of V.D3 serum levels between SLE patients and controls (P value=0.0001).This is in agreement with Meza-Meza et al., who reported that Vitamin D deficiency is more common in people with systemic lupus erythematosus (SLE) than in healthy people 33.
The laboratory investigations in total (Urea, creatinine, ESR, hemoglobin, and WBC) show an insignificant correlation with TLR7. Studies reported that TLRs, found on both leukocytes and resident renal cells, play a role in the start of glomerulonephritis and the progression of kidney injury by bridging the gap between innate and adaptive immune responses 34,35. Other studies found a link between B lymphocyte infiltration in the kidneys and glomerulonephritis, more significant activity and chronicity indices, and higher serum creatinine levels, highlighting the prognostic relevance of tubulointerstitial involvement 36.
CONCLUSIONS
The results suggested that female gender and age play a role in the etiology of SLE. Increasing TLR7 serum levels in patients compared to control indicate that TLR7 indicates the onset of the disease. There was no evidence of a correlation between TLR7 serum levels and any clinical signs or (laboratory investigations) in this study.
Acknowledgments: The authors acknowledge the contribution of the medical staff in the Rheumatology Clinic of Baghdad Teaching Hospital and appreciate the facilities introduced by the University of Baghdad\ College of Science and Department of Biotechnology.
REFERENCES
1. Basta F, Fasola F, Triantafyllias K, Schwarting A. Systemic Lupus Erythematosus (SLE) Therapy: The Old and the New. Rheumatol Ther. 2020 Sep 1 [cited 2022 Apr 17];7(3):433–46.
2. She Z, Li C, Wu F, Mao J, Xie M, Hun M, et al. The Role of B1 Cells in Systemic Lupus Erythematosus. Front Immunol. 2022 Mar 28 [cited 2022 Apr 17];13.
3. González LA, Ugarte-Gil MF, Alarcón GS. Systemic lupus erythematosus: The search for the ideal biomarker. Lupus. 2021 Feb 1 [cited 2022 Apr 17];30(2):181–203.
4. Chen JQ, Szodoray P, Zeher M. Toll-Like Receptor Pathways in Autoimmune Diseases. Clin Rev Allergy Immunol. 2016 Feb 1;50(1):1–17.
5. Bengtsson AA, Rönnblom L. Role of interferons in SLE. Best Pract Res Clin Rheumatol. 2017 Jun 1;31(3):415–28.
6. Yap DYH, Chan TM. B Cell Abnormalities in Systemic Lupus Erythematosus and Lupus Nephritis—Role in Pathogenesis and Effect of Immunosuppressive Treatments. Int J Mol Sci 2019, Vol 20, Page 6231 [Internet]. 2019 Dec 10 [cited 2022 Apr 17];20(24):6231.
7. Karrar S, Cunninghame Graham DS. Abnormal B Cell Development in Systemic Lupus Erythematosus: What the Genetics Tell Us. Arthritis Rheumatol (Hoboken, NJ) [Internet]. 2018 Apr 1 [cited 2022 Apr 17];70(4):496–507.
8. Fillatreau S, Manfroi B, Dörner T. Toll-like receptor signalling in B cells during systemic lupus erythematosus. Nat Rev Rheumatol [Internet]. 2021 Feb 1 [cited 2022 Apr 17];17(2):98–108.
9. Souyris M, Cenac C, Azar P, Daviaud D, Canivet A, Grunenwald S, et al. TLR7 escapes X chromosome inactivation in immune cells. Sci Immunol [Internet]. 2018 [cited 2022 Apr 17];3(19).
10. Mustafa R. et al. Impact of Gene Expression of TLR4 TLR7 and TLR9 in Children with Acute Lymphocytic Leukemia in Basrah - Iranian Journal of War and Public Health. 2022. [cited 2022 Jul 24].
11. Salwan M. Abdulateef, Ahmad A. Majid, Mohammed A. Al-Bayer, Srwd S. Shawkat, Ahmad Tatar, Thafer T. Mohammed, Firas M. Abdulateef, Mohammed Q. Al-Ani. Effect of aromatase inhibitors on sex differentiation and embryonic development in chicks. Veterinary Medicine and Sciencethis.2021, 7(6), pp. 2362–2373.
12. Aringer M, Leuchten N, Johnson SR. New Criteria for Lupus. Curr Rheumatol Rep [Internet]. 2020 Jun 1 [cited 2022 Apr 17];22(6):1–8.
13. Maguire GA, Ginawi A, Lee J, Lim AYN, Wood G, Houghton S, et al. Clinical utility of ANA measured by ELISA compared with ANA measured by immunofluorescence. Rheumatology. 2009;48(8):1013–4.
14. McLeod, S. A. (2019). What a p-Value Tells You about Statistical Significance. Simply Psychology. - References - Scientific Research Publishing [Internet]. [cited 2022 Jun 11].
15. Narváez J. Systemic lupus erythematosus 2020. Med Clin (Barc) [Internet]. 2020 Dec 11 [cited 2022 Apr 23];155(11):494–501.
16. Morawski PA, Bolland S. Expanding the B Cell-Centric View of Systemic Lupus Erythematosus. Trends Immunol. 2017 May 1;38(5):373–82.
17. Moulton VR, Suarez-Fueyo A, Meidan E, Li H, Mizui M, Tsokos GC. Pathogenesis of Human Systemic Lupus Erythematosus: A Cellular Perspective. Trends Mol Med [Internet]. 2017 Jul 1 [cited 2022 Apr 23];23(7):615–35.
18. Al-Sarray ZA, Izzat ;, Al-Rayahi A, Al-Hafidh AH, Dwayyikh AT. Serum Protein Electrophoresis in Iraqi Systemic lupus Erythematous Patient. J Med Sci. 2(1):2020.
19. Ohta A, Nagai M, Nishina M, Tomimitsu H, Kohsaka H. Age at onset and gender distribution of systemic lupus erythematosus, polymyositis/dermatomyositis, and systemic sclerosis in Japan. Mod Rheumatol [Internet]. 2013 Jul [cited 2022 Apr 24];23(4):759–64.
20. Rees F, Doherty M, Grainge MJ, Lanyon P, Zhang W. The worldwide incidence and prevalence of systemic lupus erythematosus: a systematic review of epidemiological studies. Rheumatology [Internet]. 2017 Nov 1 [cited 2022 Jun 10];56(11):1945–61.
21. Schwartzman-Morris J, Putterman C. Gender differences in the pathogenesis and outcome of lupus and of lupus nephritis. Clin Dev Immunol. 2012;2012.
22. M. Ajeel, A.; A. Mehdi, L. . EFFECT OF ERUCA SATIVA SEEDS POWDER AS FEED SUPPLEMENTATION ON SOME PHYSIOLOGICAL TRAITS OF MALE LAMBS. JLSAR 2020, 1, 20-30..
23. Nusbaum JS, Mirza I, Shum J, Freilich RW, Cohen RE, Pillinger MH, et al. Sex Differences in Systemic Lupus Erythematosus: Epidemiology, Clinical Considerations, and Disease Pathogenesis. Mayo Clin Proc [Internet]. 2020 Feb 1 [cited 2022 Apr 24];95(2):384–94.
24. Celhar T, Lu HK, Benso L, Rakhilina L, Lee HY, Tripathi S, et al. TLR7 protein expression in mild and severe lupus-prone models is regulated in a leukocyte, genetic, and IRAK4 dependent manner. Front Immunol [Internet]. 2019 [cited 2022 Apr 26];10(JULY).
25. Wang T, Marken J, Chen J, Tran VB, Li QZ, Li M, et al. High TLR7 expression drives the expansion of CD19+CD24HiCD38hi transitional B cells and autoantibody production in SLE patients. Front Immunol. 2019;10(JUN):1243.
26. Lyn-Cook BD, Xie C, Oates J, Treadwell E, Word B, Hammons G, et al. Increased expression of Toll-like receptors (TLRs) 7 and 9 and other cytokines in systemic lupus erythematosus (SLE) patients: ethnic differences and potential new targets for therapeutic drugs. Mol Immunol [Internet]. 2014 [cited 2022 Apr 27];61(1):38–43.
27. Nashi RA, Shmerling RH. Antinuclear Antibody Testing for the Diagnosis of Systemic Lupus Erythematosus. Med Clin North Am [Internet]. 2021 Mar 1 [cited 2022 Jun 19];105(2):387–96.
28. Aringer M, Johnson SR. Systemic Lupus Erythematosus Classification and Diagnosis. Rheum Dis Clin North Am [Internet]. 2021 Aug 1 [cited 2022 Apr 25];47(3):501–11.
29. Pisetsky DS, Lipsky PE. New insights into the role of antinuclear antibodies in systemic lupus erythematosus. Nat Rev Rheumatol [Internet]. 2020 Oct 1 [cited 2022 May 28];16(10):565.
30. Noori A, M. Jawad A, A.Jassim N, I. Gorial F. Prevalence of Antiphospholipid Antibodies in Sample of Iraqi Patients with Systemic Lupus Erythematosus: A Cross Sectional Study. Am J Clin Med Res. 2013 Oct 3;1(4):61–4.
31. Wang T, Marken J, Chen J, Tran VB, Li QZ, Li M, et al. High TLR7 expression drives the expansion of CD19+CD24HiCD38hi transitional B cells and autoantibody production in SLE patients. Front Immunol [Internet]. 2019 [cited 2022 Apr 28];10(JUN):1243.
32. F. T. Al-Rawi, Y. T. Abdul-Rahaman , Abdullah I.Noaman , Th. T. Mohammed, S. M Abdulateef, Nadia Jebril and KI. Mahmud. Role of ascorbic acid and appetite stimulants on a few blood serum biochemical characteristics in pregnant Iraqi ewes under heat stress. Revis Bionatura. 2022;7(4) 6. http://dx.doi.org/10.21931/RB/2022.07.04.6.
33. Meza-Meza MR, Muñoz-Valle JF, Ruiz-Ballesteros AI, Vizmanos-Lamotte B, Parra-Rojas I, Martínez-López E, et al. Association of High Calcitriol Serum Levels and Its Hydroxylation Efficiency Ratio with Disease Risk in SLE Patients with Vitamin D Deficiency. J Immunol Res. 2021;2021.
34. Conti F, Spinelli FR, Truglia S, Miranda F, Alessandri C, Ceccarelli F, et al. Kidney Expression of Toll Like Receptors in Lupus Nephritis: Quantification and Clinicopathological Correlations. Mediators Inflamm [Internet]. 2016 [cited 2022 Apr 29];2016.
35. =Meza-Meza MR, Muñoz-Valle JF, Ruiz-Ballesteros AI, Vizmanos-Lamotte B, Parra-Rojas I, Martínez-López E, et al. Association of High Calcitriol Serum Levels and Its Hydroxylation Efficiency Ratio with Disease Risk in SLE Patients with Vitamin D Deficiency. J Immunol Res [Internet]. 2021 [cited 2022 Apr 29];2021.
36. Chang A, Henderson SG, Brandt D, Liu N, Guttikonda R, Hsieh C, et al. In situ B cell-mediated immune responses and tubulointerstitial inflammation in human lupus nephritis. J Immunol [Internet]. 2011 Feb 1 [cited 2022 Apr 29];186(3):1849–60.
Received: 10 February 2023/ Accepted: 15 May 2023 / Published:15 June 2023
Citation: Ratib B A, Saud A M. Relationship between Toll-like Receptors and Pathogenesis of Systemic Lupus Erythematosus. Revis Bionatura 2023;8 (2) 28. http://dx.doi.org/10.21931/RB/2023.08.02.28