2022.07.02.18
Files > Volume 7 > Vol 7 No 2 2022
Comparison between immune-chromatography (ICT) and ELISA techniques for detection of anti-HAV antibodies among patients suspected to be infected with Hepatitis A virus (HAV)

Fatima Salih Hussein1 , Najat Abdeal-Qadir Zaman2 , Hajir Ali Shareef 3*
1,2,3 Department of biology, College of Science, University of Kirkuk. Irak
*Corresponding author Email: [email protected].
Available from: http://dx.doi.org/10.21931/RB/2022.07.02.18
ABSTRACT
Infection with Hepatitis A virus (HAV) is a significant cause of acute hepatitis, posing an important public health problem worldwide. This study aimed to compare the efficiency of the immune-chromatography test and the enzyme-linked immunosorbent assay (ELISA) in detecting infection with hepatitis A virus (HAV). For this purpose, 5 ml of blood was collected from 176 patients (92 males and 84 females) who attended the virology unit at Kirkuk General Hospital and the serological examination unit at the pediatric hospital, as well as private clinics in Kirkuk city for the presence of clinical signs or complaint directed towards infection doubt with hepatitis A virus (HAV), during the period between March 2020 and December 2021. The seropositive rate of anti –Hepatitis A immunoglobulin M antibody was 46(26.13%) of total patients of the study, while the ratio of the seronegative of HAV was 90(51.13%). The percentage of false-positive and false-negative results by immune-chromatography (ICT) was 34(19.38%) and 6(3.4%). These findings suggest that the fast test (ICT) is not a suitable screening test for detecting specific antibodies to the hepatitis A virus due to the high frequency of false-negative results caused by the test's low sensitivity and negative predictive value. This emphasizes employing ELISA or PCR methods to confirm hepatitis A virus diagnosis in public hospitals. Although ICTs are cheap, they alone are not useful in diagnosing and deciding treatment for patients infected with Hepatitis A virus, so it is recommended to use the ELISA test to confirm the diagnosis of infection and identify the Hepatitis A virus in public hospitals, healthcare units and blood transfusion centers.
Keywords. Hepatitis A virus, Seroprevalence, immuno-chromatographic test, ELISA test, IgM
INTRODUCTION
Hepatitis is a significant health problem in both developing and developed countries. An estimated 1.4 million clinical cases of hepatitis A occur worldwide every year1. Hepatitis A is an acute, necro-inflammatory liver infection caused by the hepatitis A virus (HAV)2. Hepatitis A virus (HAV), a small, non-enveloped with a single-stranded RNA genome, belongs to the Hepatovirus genus and is a member of the Picornaviridae family 3,4. Hepatitis A virus is acquired during early childhood. It is transmitted by a fecal-oral method which happens either by direct contact with feces or indirectly by ingestion of food or water contaminated by fecal matter of the infected persons5. The clinical course of HAV infection is age-dependent and ranges from asymptomatic (commonly in children aged ≤ 5 years) to acute symptomatic hepatitis, with higher severity of disease in the older population6. The common symptoms of hepatitis infection include fever, nausea, vomiting, anorexia, general fatigue, and abdominal pain where the liver is located. Jaundice, leading to change the urine color to dark orange and stool to light yellow or similar to clay color7,8.
Accurate detection of the virus is essential for controlling the transmission of the virus; for this reason, it is necessary to validate detection methods before allowing their use in diagnostic laboratories9. Different ways are used to diagnose hepatitis, including ICT, ELISA, and PCR. In several developing countries, rapid diagnostic tests such as ICT are widely used to detect hepatitis B and C virus for diagnosing and screening acute and chronic infections9. The current study aimed to determine the seroprevalence of HAV and compare ICT and ELISA in detecting cases of HAV, in addition to determining the percentage of a false positive and false negative in ICT tests through a statistical study of these results
MATERIALS AND METHOD
A total of 176 patients of both sexes (92 males and 84 females) were suspected of being infected with hepatitis A virus from those attending Kirkuk General Hospital (virus unit), Pediatric Hospital (serology unit) and specialized outpatient clinics in Kirkuk-Iraq for the period from March 2020 to December 2021. 5 ml venous blood was collected from patients in dry plane tubes, then centrifuged at 3000 rpm for 3 minutes to obtain serum kept in Eppendorf tubes at -20°c. Patients whose ages ranged between (1-60) years were screened for HAV using Immuno-chromatographic (ICT) kit (CTK Biotech Inc: USA) and ELISA (WANTAI Bio-Pharm: China) technique according to manufacturer instructions.
Statistical analysis:
Data was analyzed Statistically using SPPS version 20 . The Chi-square test was used to find the difference between study variables (ages and sex). The p-value is less than 0.01were considered significant.
RESULTS AND DISCUSSION
Table (1) show the ratio of the prevalence of anti-HAV-IgM in study patients by using both tests (ICT and ELISA); out of the total 176 study cases, 46 (26.13%) were the seropositive case (ICT positive / ELISA positive), 90 (51.13%) were the seronegative case (ICT negative ̸ ELISA negative), and 6 (3.4%) cases were false seronegative (ICT negative / ELISA positive). Finally, 34 (19.38%) subjects were false seropositive in the ICT test (ICT positive / ELISA negative).

Table 1. The prevalence rate of Anti-HAV-IgM among stupatients using ICT and ELISA.
Both ICT and ELISA tests were conducted on the study cases to show HAV prevalence in different age groups. The results in a table (2) showed that the infection rate was higher in the age group (1-10) years, reaching 30(17.04%) with a false seronegative rate of 6(3.4%) in the ICT test and false positivity at 18(10.23%), meaning that the total seropositive rate amounted to (20.44%) compared to the infection rate in the age group (11-20) years, which amounted to (9.09%) and the seropositive rate false 6(3.41%). The statistical analysis results showed significant differences between the age groups at a p-value <0.01, while no cases of infection were recorded in the older age groups.
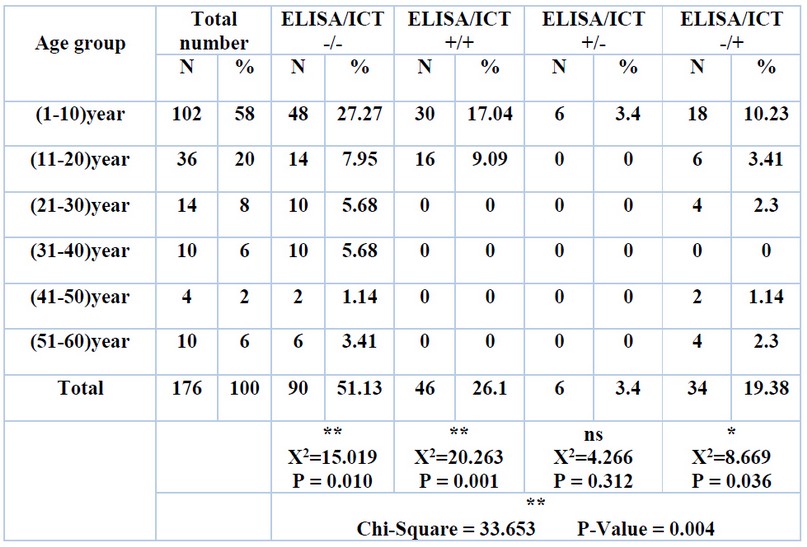
Table 2. The prevalence rate of anti-HAV-IgM among patients according to age group using ICT and ELISA.
The prevalence of hepatitis A virus (HAV) infection and its relationship with sex were also studied using both tests. The results in the table (3) showed that the prevalence of HAV infection was higher in female patients, 24(13.6%) of the total study patients (with a rate of false seronegative 2(1.14%) in the ICT test), compared to 22(12.5%) in male patients (with a rate of false seronegative 4(2.3%).
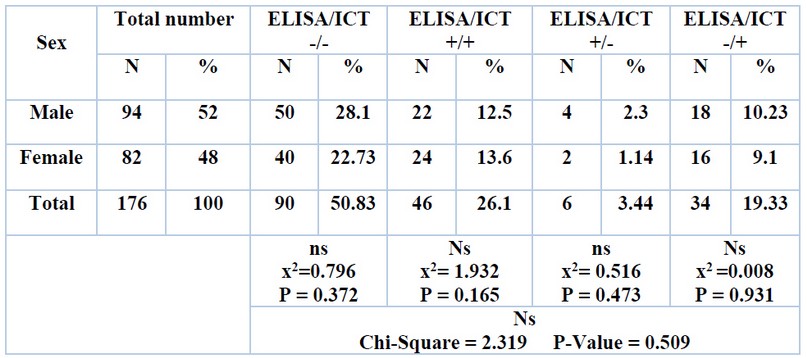
Table 3. Seroprevalence rate of anti-HAV-IgM among patients according to sex group using ICT and ELISA.
Hepatitis A viruses of different types spread very quickly in the community, so the availability of appropriate screening techniques to detect possible infection with these viruses in public hospitals can contribute significantly to the promotion of these viruses, as the confirmation of the diagnosis of hepatitis virus infection based on several immunological, molecular and histological tests. Immunological techniques to detect specific antibodies in serum include enzyme-linked immunosorbent assay (ELISA) test and rapid methods. These methods are inexpensive and available compared to molecular and histological methods that are very expensive and unavailable, especially in economically poor countries10.
The current study showed that the prevalence rate of HAV in the study patients was (26.13%) in the ICT test, compared to (29.53%), in the ELISA test, which indicates that (3.4%) of the study patients were negative in the ICT test appeared optimistic in the ELISA test. These results show that rapid tests such as ICT that are used to detect antibodies against hepatitis A virus in serum are not considered ideal screening tests because they do not predict the accurate picture of hepatitis A virus prevalence due to the high rates of false seronegative results due to the low sensitivity and specificity of these tests compared to ELISA test, which has high sensitivity and specificity11,12.
Hepatitis A virus infection is detected in some hospitals by using rapid tests. However, those tests are sensitive and specific. The possibility of some false negative or positive results cannot be ignored, as was proven in the results of the current study, which reinforces the necessity of using the ELISA test for its superiority in terms of sensitivity and specificity over the ICT test in investigating the spread of HAV cases in public hospitals.
False-negative and positive results were evaluated in the ICT test, as the current study indicated that the percentage of false-negative results in the ICT test was large (3.4%). This could be attributed to a decrease in sensitivity caused by the difficulty of detecting antibodies with low concentrations and poor affinity; compared to ELISA, the current study results agreed with other studies in the world13,10,14,15.
CONCLUSIONS
Although ICTs are cheap, they alone do not help diagnose and decide treatment for patients infected with Hepatitis A virus, so it is recommended to use the ELISA test to confirm the diagnosis of infection and identify the HAV in public hospitals healthcare units and blood transfusion centers.
Acknowledgment:
We are thankful to the staff of Kirkuk General Hospital (virus unit), Pediatric Hospital (serology unit) and specialized outpatient clinics in Kirkuk, who helped us in sample collection.
Funds sources: Self-fund
REFERENCES
1 World Health Organization. WHO/CDS/CSR/EDC/2014. Hepatitis A. Department of Communicable Disease Surveillance and Response. Available at: http://www.who. int7csr/disease/hepatitis/HepatitisA-whocdscsredc2014-pdf, accessed on April 30. 2018.
2 Pipat ,Luksamijarulkul1, Supranee ,Tongpradit2, Pisit, Vatanasomboon3 and Fuangfa Utrarachkij1 . Sero-epidemiological study of hepatitis A virus infection among hill-trib youth and household envirmental sanitationcomunity north Thailand . J of southest Asia tromped puplic health. 2003; 34: 3.
3 Malhotra, B., Kanwar, A., Reddy, P. J., Chauhan, A., Tiwari, J., Bhargava, S., & Verma, H. N. Molecular characterization of hepatitis A virus from children hospitalized at a tertiary care centre in northwest India. The Indian journal of medical research .2018; 147(5): 507.512.
4 Thomas, Howard. C., Lok, Anna. S.F., Locarnini, Stephen. A., Zuckerman, Arie. J. Viral Hepatitis, Fourth Edition. John Wiley & Sons, Ltd. 2014; 29.30.
5 Yong, H. T. and Son, R. Hepatitis A virus – a general overview. International Food Research Journal. 2009; 16: 455.467.
6 Medić, S., Anastassopoulou, C., Milošević, V., Dragnić, N., Rajčević, S., Ristić, M., & Petrović, V. Declining seroprevalence of hepatitis A in Vojvodina, Serbia. PloS one . 2019; 14(6): e0217176.
7 Ardakani A, Soltani B, Sehat M, Namjoo S, Haji Rezaei M. Seroprevalence of antihepatitis A antibody among 1-15 year old children in KashanIran. Hepat Mon. 2013;13:e10553.
8 Turky AM, Akram W, Al-Naaimi AS. Analysis of acute viral hepatitis (A and E) in Iraq. Global J Health Sci. 2011;3:70.6.
9 Asaduzzaman M, Milon AS, Juliana FM , Islam MJ, Kabir MS .Comparison Between Rapid ICT And ELISA Tests For The Detection Of HBsAg; And Screening Of Hepatitis B Infection In Apparently Healthy Bangladeshi Outbound Staff. International Journal of Engineering and Science. 2018;7:34.39.
10 Ribeiro, de Almeida C R, Amado L A, Tourinho, R S, Pinto Lima L R, Melgaço, J G, de Almeida, A J, de Paula VS.. Accuracy of rapid test for diagnosis of hepatitis A with different infection rate settings and with predictive modeling. Future microbiology .2019; 14(3): 247.258.
11 Khan JK, Lone DS, Hameed A, Munim MR, Bhatti M, Khattak AA, Usman M; Nadeem MF, Satti HS, and Munir M . Evaluation of the performance of two rapid immunochromatographic tests for detection of hepatitis B surface antigen and anti HCV antibodies using Elisa tested samples. Annals KEMU. 2010; 16: 84.87.
12 Scheiblauer H, El‐Nageh M, Nick S, Fields H, Prince A, Diaz S. Evaluation of the performance of 44 assays used in countries with limited resources for the detection of antibodies to hepatitis C virus. Transfusion. 2006; 46(5): 708.718.
13 Hortense, RPS, Bienvenue OJ, Abdoulaye TK, Lalidia OB, Asséta K, Pierre R, Nicolas B. Sero-prevalence and Risk Factors for Hepatitis A Virus Infection among Pregnant Women at the Samandin Medical Center, Ouagadougou, Burkina Faso. Journal of Advances in Biology & Biotechnology 2019; 1-9.
14 AL-Faress Sh.Evaluation of Serological Diagnostic Tests Used in the Detection of Hepatitis C Virus (HCV) Infection. Journal of Laboratory Diagnostics. 2012; 6(6).
15 Desbois D, Vaghefi P, Savary J, Dussaix E, Roque-Afonso AM. Sensitivity of a rapid immune chromatography test for hepatitis C antibodies detection. J. Clin. Virol. 2008; 41: 129.133.
.
Received: 30 December 2021 / Accepted: 25 February 2022 / Published:15 May 2022
Citation: Salih Hussein F, Abdeal-Qadir Zaman N, Ali Shareef H. Comparison between immune-chromatography (ICT) and ELISA techniques for detection of anti-HAV antibodies among patients suspected to be infected with Hepatitis A virus (HAV). Revis Bionatura 2022;7(2) 18. http://dx.doi.org/10.21931/RB/2022.07.02.18